Bronchiolitis
| Bronchiolitis | |
|---|---|
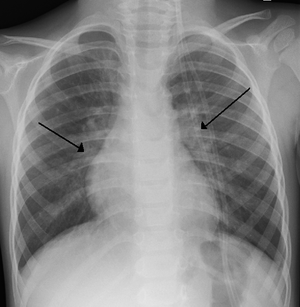 | |
| An X-ray of a child with RSV showing the typical bilateral perihilar fullness of bronchiolitis. | |
| Specialty | Emergency medicine, pediatrics |
| Symptoms | Fever, cough, runny nose, wheezing, breathing problems[1] |
| Complications | Respiratory distress, dehydration[1] |
| Usual onset | Less than 2 years old[2] |
| Causes | Viral infection (respiratory syncytial virus, human rhinovirus)[2] |
| Diagnostic method | Based on symptoms[1] |
| Differential diagnosis | Asthma, pneumonia, heart failure, allergic reaction, cystic fibrosis[1] |
| Treatment | Supportive care (oxygen, support with feeding, intravenous fluids )[3] |
| Frequency | ~20% (children less than 2)[2][1] |
| Deaths | 1% (among those hospitalized)[4] |
Bronchiolitis is blockage of the small airway in the lungs due to a viral infection.[1] It usually only occurs in children less than two years of age.[2] Symptoms may include fever, cough, runny nose, wheezing, and breathing problems.[1] More severe cases may be associated with nasal flaring, grunting, or the skin between the ribs pulling in with breathing.[1] If the child has not been able to feed properly, signs of dehydration may be present.[1]
Bronchiolitis is usually the result of infection by respiratory syncytial virus (72% of cases) or human rhinovirus (26% of cases).[2] Diagnosis is generally based on symptoms.[1] Tests such as a chest X-ray or viral testing are not routinely needed.[2] Urine testing may be considered in those with a fever.[2]
There is no specific treatment.[3] Supportive care at home is generally sufficient.[1] Occasionally hospital admission for oxygen, support with feeding, or intravenous fluids is required.[1] Tentative evidence supports nebulized hypertonic saline.[5] Evidence for antibiotics, antivirals, bronchodilators, or nebulized epinephrine is either unclear or not supportive.[6]
About 10% to 30% of children under the age of two years are affected by bronchiolitis at some point in time.[1][2] It more commonly occurs in the winter in the Northern hemisphere.[1] The risk of death among those who are admitted to hospital is about 1%.[4] Outbreaks of the condition were first described in the 1940s.[7]
Signs and symptoms
In a typical case, an infant under two years of age develops cough, wheeze, and shortness of breath over one or two days. Crackles or wheeze are typical findings on listening to the chest with a stethoscope. The infant may be breathless for several days. After the acute illness, it is common for the airways to remain sensitive for several weeks, leading to recurrent cough and wheeze.
Some signs of severe disease include:[8]
- poor feeding (less than half of usual fluid intake in preceding 24 hours)
- significantly decreased activity
- history of stopping breathing
- respiratory rate >70/min
- presence of nasal flaring and/or grunting
- severe chest wall recession (Hoover's sign)
- bluish skin
Causes
.jpg)
The term usually refers to acute viral bronchiolitis, a common disease in infancy. This is most commonly caused by respiratory syncytial virus[9] (RSV, also known as human pneumovirus). Other agents that cause this illness include human metapneumovirus, influenza, parainfluenza, coronavirus, adenovirus, rhinovirus and mycoplasma.
Children born prematurely (less than 35 weeks), with a low birth weight or who have from congenital heart disease may have higher rates of bronchiolitis and are more likely to require hospital admission. There is evidence that breastfeeding provides some protection against bronchiolitis.[10]
Diagnosis
The diagnosis is typically made by clinical examination. Chest X-ray is sometimes useful to exclude bacterial pneumonia, but not indicated in routine cases.[11]
Testing for the specific viral cause can be done but has little effect on management and thus is not routinely recommended.[11] RSV testing by direct immunofluorescence testing on nasopharyngeal aspirate had a sensitivity of 61% and specificity of 89%.[12] Identification of those who are RSV-positive can help for: disease surveillance, grouping ("cohorting") people together in hospital wards to prevent cross infection, predicting whether the disease course has peaked yet, reducing the need for other diagnostic procedures (by providing confidence that a cause has been identified).
Infants with bronchiolitis between the age of two and three months have a second infection by bacteria (usually a urinary tract infection) less than 6% of the time.[13] Preliminary studies have suggested that elevated procalcitonin levels may assist clinicians in determining the presence of bacterial coinfection, which could prevent unnecessary antibiotic use and costs.[14]
Prevention
Prevention of bronchiolitis relies strongly on measures to reduce the spread of the viruses that cause respiratory infections (that is, handwashing, and avoiding exposure to those symptomatic with respiratory infections). In addition to good hygiene an improved immune system is a great tool for prevention. One way to improve the immune system is to feed the infant with breast milk, especially during the first month of life.[15] Immunizations are available for premature infants who meet certain criteria (some cardiac and respiratory disorders) such as palivizumab (a monoclonal antibody against RSV). Passive immunization therapy requires monthly injections during winter.
Management
Treatment of bronchiolitis is usually focused on the symptoms instead of the infection itself since the infection will run its course and complications are typically from the symptoms themselves.[16] Without active treatment half of cases will go away in 13 days and 90% in three weeks.[17]
Nebulized hypertonic saline (3%) has tentative evidence of benefit.[5][6][18] Measures for which the evidence is unclear include nebulized epinephrine and nasal suctioning.[1] Treatments which the evidence does not support include salbutamol, steroids, antibiotics, antivirals, chest physiotherapy, and cool mist.[1]
Bronchodilators
Bronchodilators in children with bronchiolitis are not routinely recommended as evidence does not support a change in outcomes with such use.[19]
A 2017 review found inhaled epinephrine with corticosteroids did not change the need for hospitalization on the time spent in hospital.[20]
Non-effective
Currently other medications do not yet have evidence to support their use.[21] Ribavirin is an antiviral drug which does not appear to be effective for bronchiolitis.[22] Antibiotics are often given in case of a bacterial infection complicating bronchiolitis, but have no effect on the underlying viral infection.[23][22] Corticosteroids have no proven benefit in bronchiolitis treatment and are not advised.[22] DNAse has not been found to be effective.[24]
Epidemiology
Bronchiolitis typically affects infants and children younger than two years, principally during the fall and winter . Bronchiolitis hospitalization has a peak incidence between two and six months of age and remains a significant cause of respiratory disease during the first two years of life. It is a leading cause of hospitalization in infants and young children.[25]
See also
References
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 Friedman JN, Rieder MJ, Walton JM, Canadian Paediatric Society, Acute Care Committee, Drug Therapy and Hazardous Substances (November 2014). "Bronchiolitis: Recommendations for diagnosis, monitoring and management of children one to 24 months of age". Paediatrics & child health. 19 (9): 485–98. doi:10.1093/pch/19.9.485. PMC 4235450. PMID 25414585.
- 1 2 3 4 5 6 7 8 Schroeder, AR; Mansbach, JM (June 2014). "Recent evidence on the management of bronchiolitis". Current Opinion in Pediatrics. 26 (3): 328–33. doi:10.1097/MOP.0000000000000090. PMC 4552182. PMID 24739493.
- 1 2 Hancock, DG; Charles-Britton, B; Dixon, DL; Forsyth, KD (September 2017). "The heterogeneity of viral bronchiolitis: A lack of universal consensus definitions". Pediatric pulmonology. 52 (9): 1234–1240. doi:10.1002/ppul.23750. PMID 28672069.
- 1 2 Kendig, Edwin L.; Wilmott, Robert W.; Boat, Thomas F.; Bush, Andrew; Chernick, Victor (2012). Kendig and Chernick's Disorders of the Respiratory Tract in Children. Elsevier Health Sciences. p. 450. ISBN 1437719848.
- 1 2 Zhang, L; Mendoza-Sassi, RA; Wainwright, C; Klassen, TP (21 December 2017). "Nebulised hypertonic saline solution for acute bronchiolitis in infants". The Cochrane Database of Systematic Reviews. 12: CD006458. doi:10.1002/14651858.CD006458.pub4. PMID 29265171.
- 1 2 Brooks, CG; Harrison, WN; Ralston, SL (18 April 2016). "Association Between Hypertonic Saline and Hospital Length of Stay in Acute Viral Bronchiolitis: A Reanalysis of 2 Meta-analyses". JAMA Pediatrics. 170: 577–84. doi:10.1001/jamapediatrics.2016.0079. PMID 27088767.
- ↑ Anderson, Larry J.; Graham, Barney S. (2013). Challenges and Opportunities for Respiratory Syncytial Virus Vaccines. Springer Science & Business Media. p. 392. ISBN 9783642389191.
- ↑ BRONCHIOLITIS IN CHILDREN (Sign Guideline 91). Scottish Intercollegiate Guidelines Network. 2006. ISBN 9781905813018.
- ↑ Smyth RL, Openshaw PJ (July 2006). "Bronchiolitis". Lancet. 368 (9532): 312–22. doi:10.1016/S0140-6736(06)69077-6. PMID 16860701.
- ↑ Carbonell-Estrany X, Figueras-Aloy J (2004). "Identifying risk factors for severe respiratory syncytial virus among infants born after 33 through 35 completed weeks of gestation: different methodologies yield consistent findings". Pediatr Infect Dis J. 23 (11 Suppl): S193–201.
- 1 2 Zorc, JJ; Hall, CB (February 2010). "Bronchiolitis: recent evidence on diagnosis and management". Pediatrics. 125 (2): 342–9. doi:10.1542/peds.2009-2092. PMID 20100768.
- ↑ Bordley WC, Viswanathan M, King VJ, Sutton SF, Jackman AM, Sterling L, et al. (2004). "Diagnosis and testing in bronchiolitis: a systematic review". Arch Pediatr Adolesc Med. 158 (2): 119–26. doi:10.1001/archpedi.158.2.119. PMID 14757603.
- ↑ Ralston, S; Hill, V; Waters, A (October 2011). "Occult serious bacterial infection in infants younger than 60 to 90 days with bronchiolitis: a systematic review". Archives of Pediatrics & Adolescent Medicine. 165 (10): 951–6. doi:10.1001/archpediatrics.2011.155. PMID 21969396.
- ↑ Laham, James L.; Breheny, Patrick J.; Gardner, Brian M.; Bada, Henrietta (2014). "Procalcitonin to Predict Bacterial Coinfection in Infants With Acute Bronchiolitis". Pediatric Emergency Care. 30 (1): 11–15. doi:10.1097/PEC.0000000000000026.
- ↑ Belderbos ME, Houben ML, van Bleek GM, et al. (February 2012). "Breastfeeding modulates neonatal innate immune responses: a prospective birth cohort study". Pediatric Allergy and Immunology. 23 (1): 65–74. doi:10.1111/j.1399-3038.2011.01230.x. PMID 22103307.
- ↑ Wright, M; Mullett CJ; Piedimonte G; et al. (October 2008). "Pharmacological management of acute bronchiolitis". Veterinary Research. 4 (5): 895–903. PMC 2621418. PMID 19209271.
- ↑ Thompson, M; Vodicka, TA; Blair, PS; Buckley, DI; Heneghan, C; Hay, AD; TARGET Programme, Team (11 December 2013). "Duration of symptoms of respiratory tract infections in children: systematic review". BMJ (Clinical research ed.). 347: f7027. doi:10.1136/bmj.f7027. PMC 3898587. PMID 24335668.
- ↑ Zhang, L; Mendoza-Sassi, RA; Klassen, TP; Wainwright, C (October 2015). "Nebulized Hypertonic Saline for Acute Bronchiolitis: A Systematic Review". Pediatrics. 136 (4): 687–701. doi:10.1542/peds.2015-1914. PMID 26416925.
- ↑ Society of Hospital Medicine (2014), Pediatric Hospital Medicine: Five Things Physicians and Patients Should Question, retrieved 26 April 2014
- ↑ Kua, KP; Lee, SWH (2017). "Systematic Review and Meta-Analysis of the Efficacy and Safety of Combined Epinephrine and Corticosteroid Therapy for Acute Bronchiolitis in Infants". Frontiers in Pharmacology. 8: 396. doi:10.3389/fphar.2017.00396. PMC 5479924. PMID 28690542.
- ↑ Hartling, L; Fernandes, RM; Bialy, L; Milne, A; Johnson, D; Plint, A; Klassen, TP; Vandermeer, B (6 April 2011). "Steroids and bronchodilators for acute bronchiolitis in the first two years of life: systematic review and meta-analysis". BMJ (Clinical research ed.). 342: d1714. doi:10.1136/bmj.d1714. PMC 3071611. PMID 21471175.
- 1 2 3 Bourke, T; Shields, M (11 April 2011). "Bronchiolitis". Clinical evidence. 2011. PMID 21486501.
- ↑ Farley R, Spurling GK, Eriksson L, Del Mar CB (2014). "Antibiotics for bronchiolitis in children under two years of age". Cochrane Database of Systematic Reviews. 2014 (10): CD005189. doi:10.1002/14651858.CD005189.pub4. PMID 25300167.
- ↑ "BestBets: Do recombinant DNAse improve clinical outcome in an infant with RSV positive bronchiolitis?".
- ↑ Up to Date. www.uptodate.com Bronchiolitis in infants and children: Clinical features and diagnosis.
External links
| Classification | |
|---|---|
| External resources |
- Bronchiolitis. Patient information from NHS Choices
- "Bronchiolitis in children – A national clinical guideline" (PDF). (1.74 MB) from the Scottish Intercollegiate Guidelines Network
- Ralston, SL; Lieberthal, AS; Meissner, HC; Alverson, BK; Baley, JE; Gadomski, AM; Johnson, DW; Light, MJ; Maraqa, NF; Mendonca, EA; Phelan, KJ; Zorc, JJ; Stanko-Lopp, D; Brown, MA; Nathanson, I; Rosenblum, E; Sayles S, 3rd; Hernandez-Cancio, S (27 October 2014). "Clinical Practice Guideline: The Diagnosis, Management, and Prevention of Bronchiolitis". Pediatrics. 134 (5): e1474–502. doi:10.1542/peds.2014-2742. PMID 25349312.
| Look up bronchiolitis in Wiktionary, the free dictionary. |