Lobar pneumonia
| Lobar pneumonia | |
|---|---|
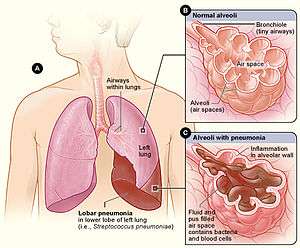 | |
| Figure A shows the location of the lungs and airways in the body. This figure also shows pneumonia affecting the lower lobe of the left lung. Figure B shows normal alveoli. Figure C shows infected alveoli. | |
| Classification and external resources | |
| Specialty | pulmonology |
| ICD-10 | J18.1 |
| ICD-9-CM | 481 |
| MeSH | D011018 |
Lobar pneumonia is a form of pneumonia that affects a large and continuous area of the lobe of a lung.[1]
It is one of the two anatomic classifications of pneumonia (the other being bronchopneumonia).
Stages

Lobar pneumonia usually has an acute progression. Classically, the disease has four stages:
- Congestion in the first 24 hours: This stage is characterized histologically by vascular engorgement, intra-alveolar fluid, small numbers of neutrophils, often numerous bacteria. Grossly, the lung is heavy and hyperemic.
- Red hepatization or consolidation: Vascular congestion persists, with extravasation of red cells into alveolar spaces, along with increased numbers of neutrophils and fibrin. The filling of airspaces by the exudate leads to a gross appearance of solidification, or consolidation, of the alveolar parenchyma. This appearance has been likened to that of the liver, hence the term "hepatization".
- Grey hepatization: Red cells disintegrate, with persistence of the neutrophils and fibrin. The alveoli still appear consolidated, but grossly the color is paler and the cut surface is drier.
- Resolution (complete recovery): The exudate is digested by enzymatic activity, and cleared by macrophages or by cough mechanism. Enzymes produced by neutrophils will liquify exudates, and this will either be coughed up in sputum or be drained via lymph.
Diagnosis

The most common organisms which cause lobar pneumonia are Streptococcus pneumoniae, also called pneumococcus, Haemophilus influenzae and Moraxella catarrhalis. Mycobacterium tuberculosis, the tubercle bacillus, may also cause lobar pneumonia if pulmonary tuberculosis is not treated promptly.
Like other types of pneumonia, lobar pneumonia can present as community acquired, in immune suppressed patients or as nosocomial infection.However, most causative organisms are of the community acquired type. Pathological specimens to be obtained for investigations include:
- Sputum for culture, AAFBS and gram stain
- Blood for full hemogram/complete blood count, ESR and other acute phase reactants
- Procalcitonin test, more specific
The identification of the infectious organism (or other cause) is an important part of modern treatment of pneumonia. The anatomical patterns of distribution can be associated with certain organisms,[2] and can help in selection of an antibiotic while waiting for the pathogen to be cultured.
References
- ↑ Cotran, Ramzi S.; Kumar, Vinay; Fausto, Nelson; Nelso Fausto; Robbins, Stanley L.; Abbas, Abul K. (2005). Robbins and Cotran pathologic basis of disease. St. Louis, Mo: Elsevier Saunders. p. 749. ISBN 0-7216-0187-1.
- ↑ "Lobar Pneumonia". Retrieved 2008-11-16.
Pathophysiology of Lobar Pneumonia The invading organism starts multiplying, thereby releasing toxins that cause inflammation and edema of the lung parenchyma. This leads to the accumulation of cellular debris within the lungs. This leads to consolidation or solidification, which is a term that is used for macroscopic or radiologic appearance of the lungs affected by pneumonia. Bacterial pneumonia is mainly classified into lobar and lo