West Nile fever
| West Nile fever | |
|---|---|
 | |
| West Nile virus | |
| Specialty | Infectious disease |
| Symptoms | None, fever, headache, vomiting, rash[1] |
| Complications | Encephalitis, meningitis[1] |
| Usual onset | 2 to 14 days post exposure[1] |
| Duration | Weeks to months[1] |
| Causes | West Nile virus spread by mosquito[1] |
| Diagnostic method | Based on symptoms and blood tests[1] |
| Prevention | Reducing mosquitoes, preventing mosquito bites[1] |
| Treatment | Supportive care (pain medication)[1] |
| Prognosis | 10% risk of death among those seriously affected[1] |
West Nile fever is a viral infection typically spread by mosquitoes.[1] In about 75% of infections people have few or no symptoms.[1] About 20% of people develop a fever, headache, vomiting, or a rash.[1] In less than 1% of people, encephalitis or meningitis occurs, with associated neck stiffness, confusion, or seizures.[1] Recovery may take weeks to months.[1] The risk of death among those in whom the nervous system is affected is about 10%.[1]
West Nile virus (WNV) is typically spread by infected mosquitoes.[1] Mosquitoes become infected when they feed on infected birds.[1] Rarely the virus is spread through blood transfusions, organ transplants, or from mother to baby during pregnancy, delivery, or breastfeeding.[1] It otherwise does not spread directly between people.[2] Risks for severe disease include age over 60 and other health problems.[1] Diagnosis is typically based on symptoms and blood tests.[1]
There is no human vaccine.[1] The best method to reduce the risk of infections is avoiding mosquito bites.[1] This may be done by eliminating standing pools of water, such as in old tires, buckets, gutters, and swimming pools.[1] Mosquito repellent, window screens, mosquito nets, and avoiding areas where mosquitoes occur may also be useful.[1][2] While there is no specific treatment, pain medications may be useful.[1]
WNV has occurred in Europe, Africa, Asia, Australia, and North America.[1] In the United States thousands of cases are reported a year, with most occurring in August and September.[3] It can occur in outbreaks of disease.[2] The virus was discovered in Uganda in 1937 and was first detected in North America in 1999.[1][2] Severe disease may also occur in horses and a vaccine for these animals is available.[2] A surveillance system in birds is useful for early detection of a potential human outbreak.[2]
Signs and symptoms
The incubation period for WNV—the amount of time from infection to symptom onset—is typically from between 2 and 15 days. Headache can be a prominent symptom of WNV fever, meningitis, encephalitis, meningoencephalitis, and it may or may not be present in poliomyelitis-like syndrome. Thus, headache is not a useful indicator of neuroinvasive disease.
- West Nile fever (WNF), which occurs in 20 percent of cases, is a febrile syndrome that causes flu-like symptoms.[4] Most characterizations of WNF generally describe it as a mild, acute syndrome lasting 3 to 6 days after symptom onset. Systematic follow-up studies of patients with WNF have not been done, so this information is largely anecdotal. In addition to a high fever, headache, chills, excessive sweating, weakness, fatigue, swollen lymph nodes, drowsiness, pain in the joints and flu-like symptoms. Gastrointestinal symptoms that may occur include nausea, vomiting, loss of appetite, and diarrhea. Fewer than one-third of patients develop a rash.
- West Nile neuroinvasive disease (WNND), which occurs in less than 1 percent of cases, is when the virus infects the central nervous system resulting in meningitis, encephalitis, meningoencephalitis or a poliomyelitis-like syndrome.[5] Many patients with WNND have normal neuroimaging studies, although abnormalities may be present in various cerebral areas including the basal ganglia, thalamus, cerebellum, and brainstem.[5]
- West Nile virus encephalitis (WNE) is the most common neuroinvasive manifestation of WNND. WNE presents with similar symptoms to other viral encephalitis with fever, headaches, and altered mental status. A prominent finding in WNE is muscular weakness (30 to 50 percent of patients with encephalitis), often with lower motor neuron symptoms, flaccid paralysis, and hyporeflexia with no sensory abnormalities.[6][7]
- West Nile meningitis (WNM) usually involves fever, headache, and stiff neck. Pleocytosis, an increase of white blood cells in cerebrospinal fluid, is also present. Changes in consciousness are not usually seen and are mild when present.
- West Nile meningoencephalitis is inflammation of both the brain (encephalitis) and meninges (meningitis).
- West Nile poliomyelitis (WNP), an acute flaccid paralysis syndrome associated with WNV infection, is less common than WNM or WNE. This syndrome is generally characterized by the acute onset of asymmetric limb weakness or paralysis in the absence of sensory loss. Pain sometimes precedes the paralysis. The paralysis can occur in the absence of fever, headache, or other common symptoms associated with WNV infection. Involvement of respiratory muscles, leading to acute respiratory failure, can sometimes occur.
- West-Nile reversible paralysis, Like WNP, the weakness or paralysis is asymmetric.[8] Reported cases have been noted to have an initial preservation of deep tendon reflexes, which is not expected for a pure anterior horn involvement.[8] Disconnect of upper motor neuron influences on the anterior horn cells possibly by myelitis or glutamate excitotoxicity have been suggested as mechanisms.[8] The prognosis for recovery is excellent.
- Nonneurologic complications of WNV infection that may rarely occur include fulminant hepatitis, pancreatitis,[9] myocarditis, rhabdomyolysis,[10] orchitis,[11] nephritis, optic neuritis[12] and cardiac dysrhythmias and hemorrhagic fever with coagulopathy.[13] Chorioretinitis may also be more common than previously thought.[14]
- Cutaneous manifestations specifically rashes, are not uncommon in WNV-infected patients; however, there is a paucity of detailed descriptions in case reports and there are few clinical images widely available. Punctate erythematous, macular, and papular eruptions, most pronounced on the extremities have been observed in WNV cases and in some cases histopathologic findings have shown a sparse superficial perivascular lymphocytic infiltrate, a manifestation commonly seen in viral exanthems. A literature review provides support that this punctate rash is a common cutaneous presentation of WNV infection.[15]
Cause
Virology

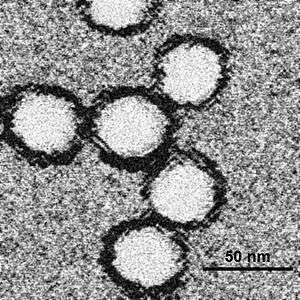
WNV is one of the Japanese encephalitis antigenic serocomplex of viruses. Image reconstructions and cryoelectron microscopy reveal a 45–50 nm virion covered with a relatively smooth protein surface. This structure is similar to the dengue fever virus; both belong to the genus Flavivirus within the family Flaviviridae. The genetic material of WNV is a positive-sense, single strand of RNA, which is between 11,000 and 12,000 nucleotides long; these genes encode seven nonstructural proteins and three structural proteins. The RNA strand is held within a nucleocapsid formed from 12-kDa protein blocks; the capsid is contained within a host-derived membrane altered by two viral glycoproteins.
Transmission
The prime method of spread of the West Nile virus (WNV) is the female mosquito. In Europe, cats were identified as being hosts for West Nile virus.[16] The important mosquito vectors vary according to area; in the United States, Culex pipiens (Eastern United States, and urban and residential areas of the United States north of 36–39°N), Culex tarsalis (Midwest and West), and Culex quinquefasciatus (Southeast) are the main vector species.[17]
The mosquito species that are most frequently infected with WNV feed primarily on birds.[18] Different species of mosquitos take a blood meal from different types of vertebrate hosts, Mosquitoes show further selectivity, exhibiting preference for different species of birds. In the United States, WNV mosquito vectors feed preferentially on members of the Corvidae and thrush family. Among the preferred species within these families are the American crow, a corvid, and the American robin (Turdus migratorius).[19]
Some species of birds develop sufficient viral levels (>~104.2 log PFU/ml;[20]) after being infected to transmit the infection to biting mosquitoes that in turn go on to infect other birds. In birds that die from WNV, death usually occurs after 4 to 6 days.[21] In mammals and several species of birds, the virus does not multiply as readily and so does not develop high viremia during infection. Mosquitoes biting such hosts are not believed to ingest sufficient virus to become infected, making them so-called dead-end hosts.[20] As a result of the differential infectiousness of hosts, the feeding patterns of mosquitoes play an important role in WNV transmission,[18][19] and they are partly genetically controlled, even within a species.
Direct human-to-human transmission initially was believed to be caused only by occupational exposure, such as in a laboratory setting,[22] or conjunctive exposure to infected blood.[23] The US outbreak identified additional transmission methods through blood transfusion,[24] organ transplant,[25] intrauterine exposure,[26] and breast feeding.[27] Since 2003, blood banks in the United States routinely screen for the virus among their donors.[28] As a precautionary measure, the UK's National Blood Service initially ran a test for this disease in donors who donate within 28 days of a visit to the United States, Canada, or the northeastern provinces of Italy, and the Scottish National Blood Transfusion Service[29] asks prospective donors to wait 28 days after returning from North America or the northeastern provinces of Italy before donating. There also have been reports of possible transmission of the virus from mother to child during pregnancy or breastfeeding or exposure to the virus in a lab, but these are rare cases and not conclusively confirmed.[30]
Recently, the potential for mosquito saliva to affect the course of WNV disease was demonstrated.[31][32][33] Mosquitoes inoculate their saliva into the skin while obtaining blood. Mosquito saliva is a pharmacological cocktail of secreted molecules, principally proteins, that can affect vascular constriction, blood coagulation, platelet aggregation, inflammation, and immunity. It clearly alters the immune response in a manner that may be advantageous to a virus.[34][35][36][37] Studies have shown it can specifically modulate the immune response during early virus infection,[38] and mosquito feeding can exacerbate WNV infection, leading to higher viremia and more severe forms of disease.[31][32][33]
Vertical transmission
Vertical transmission, the transmission of a viral or bacterial disease from the female of the species to her offspring, has been observed in various West Nile virus studies, amongst different species of mosquitoes in both the laboratory and in nature.[39] Mosquito progeny infected vertically in autumn, may potentially serve as a mechanism for WNV to overwinter and initiate enzootic horizontal transmission the following spring, although it likely plays little role in transmission in the summer and fall.[40]
Risk factors
Risk factors independently associated with developing a clinical infection with WNV include a suppressed immune system and a patient history of organ transplantation.[41] For neuroinvasive disease the additional risk factors include older age (>50+), male sex, hypertension, and diabetes mellitus.[42][43]
A genetic factor also appears to increase susceptibility to West Nile disease. A mutation of the gene CCR5 gives some protection against HIV but leads to more serious complications of WNV infection. Carriers of two mutated copies of CCR5 made up 4.0 to 4.5% of a sample of West Nile disease sufferers, while the incidence of the gene in the general population is only 1.0%.[44][45]
Diagnosis
Preliminary diagnosis is often based on the patient's clinical symptoms, places and dates of travel (if patient is from a nonendemic country or area), activities, and epidemiologic history of the location where infection occurred. A recent history of mosquito bites and an acute febrile illness associated with neurologic signs and symptoms should cause clinical suspicion of WNV.
Diagnosis of West Nile virus infections is generally accomplished by serologic testing of blood serum or cerebrospinal fluid (CSF), which is obtained via a lumbar puncture. Initial screening could be done using the ELISA technique detecting immunoglobulins in the sera of the tested individuals.
Typical findings of WNV infection include lymphocytic pleocytosis, elevated protein level, reference glucose and lactic acid levels, and no erythrocytes.
Definitive diagnosis of WNV is obtained through detection of virus-specific antibody IgM and neutralizing antibodies. Cases of West Nile virus meningitis and encephalitis that have been serologically confirmed produce similar degrees of CSF pleocytosis and are often associated with substantial CSF neutrophilia.[46] Specimens collected within eight days following onset of illness may not test positive for West Nile IgM, and testing should be repeated. A positive test for West Nile IgG in the absence of a positive West Nile IgM is indicative of a previous flavivirus infection and is not by itself evidence of an acute West Nile virus infection.[47]
If cases of suspected West Nile virus infection, sera should be collected on both the acute and convalescent phases of the illness. Convalescent specimens should be collected 2–3 weeks after acute specimens.
It is common in serologic testing for cross-reactions to occur among flaviviruses such as dengue virus (DENV) and tick-borne encephalitis virus; this necessitates caution when evaluating serologic results of flaviviral infections.[48]
Four FDA-cleared WNV IgM ELISA kits are commercially available from different manufacturers in the U.S., each of these kits is indicated for use on serum to aid in the presumptive laboratory diagnosis of WNV infection in patients with clinical symptoms of meningitis or encephalitis. Positive WNV test results obtained via use of these kits should be confirmed by additional testing at a state health department laboratory or CDC.
In fatal cases, nucleic acid amplification, histopathology with immunohistochemistry, and virus culture of autopsy tissues can also be useful. Only a few state laboratories or other specialized laboratories, including those at CDC, are capable of doing this specialized testing.
Differential diagnosis
A number of various diseases may present with symptoms similar to those caused by a clinical West Nile virus infection. Those causing neuroinvasive disease symptoms include the enterovirus infection and bacterial meningitis. Accounting for differential diagnoses is a crucial step in the definitive diagnosis of WNV infection. Consideration of a differential diagnosis is required when a patient presents with unexplained febrile illness, extreme headache, encephalitis or meningitis. Diagnostic and serologic laboratory testing using polymerase chain reaction (PCR) testing and viral culture of CSF to identify the specific pathogen causing the symptoms, is the only currently available means of differentiating between causes of encephalitis and meningitis.
Prevention

Personal protective measures can be taken to greatly reduce the risk of being bitten by an infected mosquito:
- Using insect repellent on exposed skin to repel mosquitoes. EPA-registered repellents include products containing DEET (N,N-diethylmetatoluamide) and picaridin (KBR 3023). DEET concentrations of 30% to 50% are effective for several hours. Picaridin, available at 7% and 15% concentrations, needs more frequent application. DEET formulations as high as 30% are recommended for children over two months of age.[49] Protect infants less than two months of age by using a carrier draped with mosquito netting with an elastic edge for a tight fit.
- When using sunscreen, apply sunscreen first and then repellent. Repellent should be washed off at the end of the day before going to bed.
- Wear long-sleeve shirts, which should be tucked in, long pants, socks, and hats to cover exposed skin. Insect repellents should be applied over top of protective clothing for greater protection. Do not apply insect repellents underneath clothing.
- The application of permethrin-containing (e.g., Permanone) or other insect repellents to clothing, shoes, tents, mosquito nets, and other gear for greater protection. Permethrin is not labeled for use directly on skin. Most repellent is generally removed from clothing and gear by a single washing, but permethrin-treated clothing is effective for up to five washings.
- Be aware that most mosquitoes that transmit disease are most active during twilight periods (dawn and dusk or in the evening). A notable exception is the Asian tiger mosquito, which is a daytime feeder and is more apt to be found in, or on the periphery of, shaded areas with heavy vegetation. They are now widespread in the United States, and in Florida they have been found in all 67 counties.[50]
- Staying in air-conditioned or well-screened housing, and/or sleeping under an insecticide-treated bed net. Bed nets should be tucked under mattresses and can be sprayed with a repellent if not already treated with an insecticide.
Monitoring and control
West Nile virus can be sampled from the environment by the pooling of trapped mosquitoes via ovitraps, carbon dioxide-baited light traps, and gravid traps, testing blood samples drawn from wild birds, dogs, and sentinel monkeys, as well as testing brains of dead birds found by various animal control agencies and the public.
Testing of the mosquito samples requires the use of reverse-transcriptase PCR (RT-PCR) to directly amplify and show the presence of virus in the submitted samples. When using the blood sera of wild birds and sentinel chickens, samples must be tested for the presence of WNV antibodies by use of immunohistochemistry (IHC)[51] or enzyme-linked immunosorbent assay (ELISA).[52]
Dead birds, after necropsy, or their oral swab samples collected on specific RNA-preserving filter paper card,[53][54] can have their virus presence tested by either RT-PCR or IHC, where virus shows up as brown-stained tissue because of a substrate-enzyme reaction.
West Nile control is achieved through mosquito control, by elimination of mosquito breeding sites such as abandoned pools, applying larvacide to active breeding areas, and targeting the adult population via lethal ovitraps and aerial spraying of pesticides.
Environmentalists have condemned attempts to control the transmitting mosquitoes by spraying pesticide, saying the detrimental health effects of spraying outweigh the relatively few lives that may be saved, and more environmentally friendly ways of controlling mosquitoes are available. They also question the effectiveness of insecticide spraying, as they believe mosquitoes that are resting or flying above the level of spraying will not be killed; the most common vector in the northeastern United States, Culex pipiens, is a canopy feeder.
 A carbon dioxide-baited CDC light trap at NPSmonitoring site: The highest individual light trap total for 2010 was from a trap located in a salt marsh in the Fire Island National Seashore: around 25,142 mosquitoes were collected during a 16-hour period on August 31.[55]
A carbon dioxide-baited CDC light trap at NPSmonitoring site: The highest individual light trap total for 2010 was from a trap located in a salt marsh in the Fire Island National Seashore: around 25,142 mosquitoes were collected during a 16-hour period on August 31.[55] Eggs of permanent water mosquitoes can hatch, and the larvae survive, in only a few ounces of water. Less than half the amount that may collect in a discarded coffee cup. Floodwater species lay their eggs on wet soil or other moist surfaces. Hatch time is variable for both types; under favorable circumstances (such as warm weather), the eggs of some species may hatch in as few as 1–3 days after being laid.[56]
Eggs of permanent water mosquitoes can hatch, and the larvae survive, in only a few ounces of water. Less than half the amount that may collect in a discarded coffee cup. Floodwater species lay their eggs on wet soil or other moist surfaces. Hatch time is variable for both types; under favorable circumstances (such as warm weather), the eggs of some species may hatch in as few as 1–3 days after being laid.[56] Used tires often hold stagnant water and are a breeding ground for many species of mosquitoes. Some species such as the Asian tiger mosquito prefer manmade containers, such as tires, in which to lay their eggs. The rapid spread of this aggressive daytime feeding species beyond their native range has been attributed to the used tire trade.[50][57]
Used tires often hold stagnant water and are a breeding ground for many species of mosquitoes. Some species such as the Asian tiger mosquito prefer manmade containers, such as tires, in which to lay their eggs. The rapid spread of this aggressive daytime feeding species beyond their native range has been attributed to the used tire trade.[50][57]
Treatment
Most people recover from West Nile virus without treatment. No specific treatment is available for WNV infection. In mild cases over the counter pain relievers can help ease mild headaches and muscle aches in adults. In severe cases treatment consists of supportive care that often involves hospitalization, intravenous fluids, pain medication, respiratory support, and prevention of secondary infections.
Prognosis
While the general prognosis is favorable, current studies indicate that West Nile Fever can often be more severe than previously recognized, with studies of various recent outbreaks indicating that it may take as long as 60–90 days to recover.[7][58] People with milder WNF are just as likely as those with more severe manifestations of neuroinvasive disease to experience multiple long term (>1+ years) somatic complaints such as tremor, and dysfunction in motor skills and executive functions. People with milder illness are just as likely as people with more severe illness to experience adverse outcomes.[59] Recovery is marked by a long convalescence with fatigue. One study found that neuroinvasive WNV infection was associated with an increased risk for subsequent kidney disease.[60][61]
Epidemiology
WNV was first isolated from a feverish 37-year-old woman at Omogo in the West Nile District of Uganda in 1937 during research on yellow fever virus.[62] A series of serosurveys in 1939 in central Africa found anti-WNV positive results ranging from 1.4% (Congo) to 46.4% (White Nile region, Sudan). It was subsequently identified in Egypt (1942) and India (1953), a 1950 serosurvey in Egypt found 90% of those over 40 years in age had WNV antibodies. The ecology was characterized in 1953 with studies in Egypt[63] and Israel.[64] The virus became recognized as a cause of severe human meningoencephalitis in elderly patients during an outbreak in Israel in 1957. The disease was first noted in horses in Egypt and France in the early 1960s and found to be widespread in southern Europe, southwest Asia and Australia.
The first appearance of WNV in the Western Hemisphere was in 1999[65] with encephalitis reported in humans, dogs, cats, and horses, and the subsequent spread in the United States may be an important milestone in the evolving history of this virus. The American outbreak began in College Point, Queens in New York City and was later spread to the neighboring states of New Jersey and Connecticut. The virus is believed to have entered in an infected bird or mosquito, although there is no clear evidence.[66] West Nile virus is now endemic in Africa, Europe, the Middle East, west and central Asia, Oceania (subtype Kunjin), and most recently, North America and is spreading into Central and South America.
Outbreaks of West Nile virus encephalitis in humans have occurred in Algeria (1994), Romania (1996 to 1997), the Czech Republic (1997), Congo (1998), Russia (1999), the United States (1999 to 2009), Canada (1999–2007), Israel (2000) and Greece (2010).
Epizootics of disease in horses occurred in Morocco (1996), Italy (1998), the United States (1999 to 2001), and France (2000), Mexico (2003) and Sardinia (2011).
Outdoor workers (including biological fieldworkers, construction workers, farmers, landscapers, and painters), healthcare personnel, and laboratory personnel who perform necropsies on animals are at risk of contracting WNV.[67]
In 2012, the US experienced one of its worst epidemics in which 286 people died, with the state of Texas being hard hit by this virus.[68][69]
Research
A vaccine for horses (ATCvet code: QI05AA10 (WHO)) based on killed viruses exists; some zoos have given this vaccine to their birds, although its effectiveness is unknown. Dogs and cats show few if any signs of infection. There have been no known cases of direct canine-human or feline-human transmission; although these pets can become infected, it is unlikely they are, in turn, capable of infecting native mosquitoes and thus continuing the disease cycle.[70] AMD3100, which had been proposed as an antiretroviral drug for HIV, has shown promise against West Nile encephalitis. Morpholino antisense oligos conjugated to cell penetrating peptides have been shown to partially protect mice from WNV disease.[71] There have also been attempts to treat infections using ribavirin, intravenous immunoglobulin, or alpha interferon.[72] GenoMed, a U.S. biotech company, has found that blocking angiotensin II can treat the "cytokine storm" of West Nile virus encephalitis as well as other viruses.[73]
A vaccine called Chimerivax-WNV is being actively researched and has undergone phase II Clinical trials in 2011.[74][75]
References
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 "General Questions About West Nile Virus". www.cdc.gov. 19 October 2017. Archived from the original on 26 October 2017. Retrieved 26 October 2017.
- 1 2 3 4 5 6 "West Nile virus". World Health Organization. July 2011. Archived from the original on 18 October 2017. Retrieved 28 October 2017.
- ↑ "Final Cumulative Maps and Data | West Nile Virus | CDC". www.cdc.gov. 24 October 2017. Archived from the original on 27 October 2017. Retrieved 28 October 2017.
- ↑ Olejnik E (1952). "Infectious adenitis transmitted by Culex molestus". Bull Res Counc Isr. 2: 210–1.
- 1 2 Davis LE, DeBiasi R, Goade DE, et al. (Sep 2006). "West Nile virus neuroinvasive disease". Ann Neurol. 60 (3): 286–300. doi:10.1002/ana.20959. PMID 16983682.
- ↑ Flores Anticona EM, Zainah H, Ouellette DR, Johnson LE (2012). "Two case reports of neuroinvasive west nile virus infection in the critical care unit". Case Rep Infect Dis. 2012: 839458. doi:10.1155/2012/839458. PMC 3433121. PMID 22966470.
- 1 2 Carson PJ, Konewko P, Wold KS, et al. (2006). "Long-term clinical and neuropsychological outcomes of West Nile virus infection" (PDF). Clin. Infect. Dis. 43 (6): 723–30. doi:10.1086/506939. PMID 16912946.
- 1 2 3 Mojumder, D. K., Agosto, M., Wilms, H.; et al. (March 2014). "Is initial preservation of deep tendon reflexes in West Nile Virus paralysis a good prognostic sign?". Neurology Asia. 19 (1): 93–97. PMC 4229851. PMID 25400704.
- ↑ Asnis DS, Conetta R, Teixeira AA, Waldman G, Sampson BA (March 2000). "The West Nile Virus outbreak of 1999 in New York: the Flushing Hospital experience". Clin. Infect. Dis. 30 (3): 413–8. doi:10.1086/313737. PMID 10722421.
- ↑ Montgomery SP, Chow CC, Smith SW, Marfin AA, O'Leary DR, Campbell GL (2005). "Rhabdomyolysis in patients with west nile encephalitis and meningitis". Vector-Borne and Zoonotic Diseases. 5 (3): 252–7. doi:10.1089/vbz.2005.5.252. PMID 16187894.
- ↑ Smith RD, Konoplev S, DeCourten-Myers G, Brown T (February 2004). "West Nile virus encephalitis with myositis and orchitis". Hum. Pathol. 35 (2): 254–8. doi:10.1016/j.humpath.2003.09.007. PMID 14991545.
- ↑ Anninger WV, Lomeo MD, Dingle J, Epstein AD, Lubow M (2003). "West Nile virus-associated optic neuritis and chorioretinitis". Am. J. Ophthalmol. 136 (6): 1183–5. doi:10.1016/S0002-9394(03)00738-4. PMID 14644244.
- ↑ Paddock CD, Nicholson WL, Bhatnagar J, et al. (June 2006). "Fatal hemorrhagic fever caused by West Nile virus in the United States". Clin. Infect. Dis. 42 (11): 1527–35. doi:10.1086/503841. PMID 16652309.
- ↑ Shaikh S, Trese MT (2004). "West Nile virus chorioretinitis". Br J Ophthalmol. 88 (12): 1599–60. doi:10.1136/bjo.2004.049460. PMC 1772450. PMID 15548822.
- ↑ Anderson RC, Horn KB, Hoang MP, Gottlieb E, Bennin B (November 2004). "Punctate exanthem of West Nile Virus infection: report of 3 cases". J. Am. Acad. Dermatol. 51 (5): 820–3. doi:10.1016/j.jaad.2004.05.031. PMID 15523368.
- ↑ Rijks, J.M.; Cito, F.; Cunningham, A.A.; Rantsios, A.T.; Giovannini, A. (2016). "Disease Risk Assessments Involving Companion Animals: an Overview for 15 Selected Pathogens Taking a European Perspective". Journal of Comparative Pathology. 155 (1): S75–S97. doi:10.1016/j.jcpa.2015.08.003. ISSN 0021-9975.
- ↑ Hayes EB, Komar N, Nasci RS, Montgomery SP, O'Leary DR, Campbell GL (2005). "Epidemiology and transmission dynamics of West Nile virus disease". Emerging Infect. Dis. 11 (8): 1167–73. doi:10.3201/eid1108.050289a. PMC 3320478. PMID 16102302. Archived from the original on 2011-07-29.
- 1 2 Kilpatrick, A.M. (2011). "Globalization, land use, and the invasion of West Nile virus". Science. 334 (6054): 323–327. doi:10.1126/science.1201010. PMC 3346291. PMID 22021850.
- 1 2 Kilpatrick, AM, P Daszak, MJ Jones, PP Marra, LD Kramer (2006). "Host heterogeneity dominates West Nile virus transmission". Proceedings of the Royal Society B: Biological Sciences. 273 (1599): 2327–2333. doi:10.1098/rspb.2006.3575. PMC 1636093. PMID 16928635.
- 1 2 Kilpatrick, AM, SL LaDeau, PP Marra (2007). "Ecology of West Nile virus transmission and its impact on birds in the western hemisphere". Auk. 124 (4): 1121–1136. doi:10.1642/0004-8038(2007)124[1121:eownvt]2.0.co;2.
- ↑ Komar, N, S Langevin, S Hinten, N Nemeth, E Edwards, D Hettler, B Davis, R Bowen, M Bunning (2003). "Experimental infection of North American birds with the New York 1999 strain of West Nile virus". Emerging Infectious Diseases. 9 (3): 311–322. doi:10.3201/eid0903.020628. PMC 2958552. PMID 12643825.
- ↑ Centers for Disease Control and Prevention (CDC) (2002). "Laboratory-acquired West Nile virus infections—United States, 2002". MMWR Morb. Mortal. Wkly. Rep. 51 (50): 1133–5. PMID 12537288.
- ↑ Fonseca K, Prince GD, Bratvold J, et al. (2005). "West Nile virus infection and conjunctive exposure". Emerging Infect. Dis. 11 (10): 1648–9. doi:10.3201/eid1110.040212. PMC 3366727. PMID 16355512.
- ↑ Centers for Disease Control and Prevention (CDC) (2002). "Investigation of blood transfusion recipients with West Nile virus infections". MMWR Morb. Mortal. Wkly. Rep. 51 (36): 823. PMID 12269472.
- ↑ Centers for Disease Control and Prevention (CDC) (2002). "West Nile virus infection in organ donor and transplant recipients—Georgia and Florida, 2002". MMWR Morb. Mortal. Wkly. Rep. 51 (35): 790. PMID 12227442.
- ↑ Centers for Disease Control and Prevention (CDC) (2002). "Intrauterine West Nile virus infection—New York, 2002". MMWR Morb. Mortal. Wkly. Rep. 51 (50): 1135–6. PMID 12537289.
- ↑ Centers for Disease Control and Prevention (CDC) (2002). "Possible West Nile virus transmission to an infant through breast-feeding—Michigan, 2002". MMWR Morb. Mortal. Wkly. Rep. 51 (39): 877–8. PMID 12375687.
- ↑ Centers for Disease Control and Prevention (CDC) (2003). "Detection of West Nile virus in blood donations—United States, 2003". MMWR Morb. Mortal. Wkly. Rep. 52 (32): 769–72. PMID 12917583. Archived from the original on 2017-06-25.
- ↑ West Nile Virus. Scottish National Blood Transfusion Service.
- ↑ "West Nile virus". Mayo Clinic. Archived from the original on 26 October 2017. Retrieved 25 October 2017.
- 1 2 Schneider BS, McGee CE, Jordan JM, Stevenson HL, Soong L, Higgs S (2007). Baylis, Matthew, ed. "Prior exposure to uninfected mosquitoes enhances mortality in naturally-transmitted West Nile virus infection". PLoS ONE. 2 (11): e1171. doi:10.1371/journal.pone.0001171. PMC 2048662. PMID 18000543.
- 1 2 Styer LM, Bernard KA, Kramer LD (2006). "Enhanced early West Nile virus infection in young chickens infected by mosquito bite: effect of viral dose". Am. J. Trop. Med. Hyg. 75 (2): 337–45. PMID 16896145.
- 1 2 Schneider BS, Soong L, Girard YA, Campbell G, Mason P, Higgs S (2006). "Potentiation of West Nile encephalitis by mosquito feeding". Viral Immunol. 19 (1): 74–82. doi:10.1089/vim.2006.19.74. PMID 16553552.
- ↑ Wasserman HA, Singh S, Champagne DE (2004). "Saliva of the Yellow Fever mosquito, Aedes aegypti, modulates murine lymphocyte function". Parasite Immunol. 26 (6–7): 295–306. doi:10.1111/j.0141-9838.2004.00712.x. PMID 15541033.
- ↑ Limesand KH, Higgs S, Pearson LD, Beaty BJ (2003). "Effect of mosquito salivary gland treatment on vesicular stomatitis New Jersey virus replication and interferon alpha/beta expression in vitro". J. Med. Entomol. 40 (2): 199–205. doi:10.1603/0022-2585-40.2.199. PMID 12693849.
- ↑ Wanasen N, Nussenzveig RH, Champagne DE, Soong L, Higgs S (2004). "Differential modulation of murine host immune response by salivary gland extracts from the mosquitoes Aedes aegypti and Culex quinquefasciatus". Med. Vet. Entomol. 18 (2): 191–9. doi:10.1111/j.1365-2915.2004.00498.x. PMID 15189245.
- ↑ Zeidner NS, Higgs S, Happ CM, Beaty BJ, Miller BR (1999). "Mosquito feeding modulates Th1 and Th2 cytokines in flavivirus susceptible mice: an effect mimicked by injection of sialokinins, but not demonstrated in flavivirus resistant mice". Parasite Immunol. 21 (1): 35–44. doi:10.1046/j.1365-3024.1999.00199.x. PMID 10081770.
- ↑ Schneider BS, Soong L, Zeidner NS, Higgs S (2004). "Aedes aegypti salivary gland extracts modulate anti-viral and TH1/TH2 cytokine responses to sindbis virus infection". Viral Immunol. 17 (4): 565–73. doi:10.1089/vim.2004.17.565. PMID 15671753.
- ↑ Bugbee, LM; Forte LR (September 2004). "The discovery of West Nile virus in overwintering Culex pipiens (Diptera: Culicidae) mosquitoes in Lehigh County, Pennsylvania". Journal of the American Mosquito Control Association. 20 (3): 326–7. PMID 15532939.
- ↑ Goddard LB, Roth AE, Reisen WK, Scott TW (November 2003). "Vertical transmission of West Nile Virus by three California Culex (Diptera: Culicidae) species". J. Med. Entomol. 40 (6): 743–6. doi:10.1603/0022-2585-40.6.743. PMID 14765647.
- ↑ Kumar D, Drebot MA, Wong SJ, et al. (2004). "A seroprevalence study of West Nile virus infection in solid organ transplant recipients". Am. J. Transplant. 4 (11): 1883–8. doi:10.1111/j.1600-6143.2004.00592.x. PMID 15476490.
- ↑ Jean CM, Honarmand S, Louie JK, Glaser CA (December 2007). "Risk factors for West Nile virus neuroinvasive disease, California, 2005". Emerging Infect. Dis. 13 (12): 1918–20. doi:10.3201/eid1312.061265. PMC 2876738. PMID 18258047.
- ↑ Kumar D, Drebot MA, Wong SJ, et al. (2004). "A seroprevalence study of west nile virus infection in solid organ transplant recipients". Am. J. Transplant. 4 (11): 1883–8. doi:10.1111/j.1600-6143.2004.00592.x. PMID 15476490.
- ↑ Glass, WG; Lim JK; Cholera R; Pletnev AG; Gao JL; Murphy PM (October 17, 2005). "Chemokine receptor CCR5 promotes leukocyte trafficking to the brain and survival in West Nile virus infection". Journal of Experimental Medicine. 202 (8): 1087–98. doi:10.1084/jem.20042530. PMC 2213214. PMID 16230476.
- ↑ Glass, WG; McDermott DH; Lim JK; Lekhong S; Yu SF; Frank WA; Pape J; Cheshier RC; Murphy PM (January 23, 2006). "CCR5 deficiency increases risk of symptomatic West Nile virus infection". Journal of Experimental Medicine. 203 (1): 35–40. doi:10.1084/jem.20051970. PMC 2118086. PMID 16418398.
- ↑ Tyler KL, Pape J, Goody RJ, Corkill M, Kleinschmidt-DeMasters BK (February 2006). "CSF findings in 250 patients with serologically confirmed West Nile virus meningitis and encephalitis". Neurology. 66 (3): 361–5. doi:10.1212/01.wnl.0000195890.70898.1f. PMID 16382032.
- ↑ "2012 DOHMH Advisory #8: West Nile Virus" (PDF). New York City Department of Health and Mental Hygiene. June 28, 2012. Archived (PDF) from the original on December 3, 2013.
- ↑ Papa A, Karabaxoglou D, Kansouzidou A (October 2011). "Acute West Nile virus neuroinvasive infections: cross-reactivity with dengue virus and tick-borne encephalitis virus". J. Med. Virol. 83 (10): 1861–5. doi:10.1002/jmv.22180. PMID 21837806.
- ↑ American Academy of Pediatrics (8 August 2012). "Choosing an Insect Repellent for Your Child". healthychildren.org. Archived from the original on 27 August 2016. Retrieved 24 August 2016.
- 1 2 Rios L, Maruniak JE (October 2011). "Asian Tiger Mosquito, Aedes albopictus (Skuse) (Insecta: Diptera: Culicidae)". Department of Entomology and Nematology, University of Florida. EENY-319. Archived from the original on 2012-09-26.
- ↑ Jozan, M; Evans R; McLean R; Hall R; Tangredi B; Reed L; Scott J (Fall 2003). "Detection of West Nile virus infection in birds in the United States by blocking ELISA and immunohistochemistry". Vector-Borne and Zoonotic Diseases. 3 (3): 99–110. doi:10.1089/153036603768395799. PMID 14511579.
- ↑ Hall, RA; Broom AK; Hartnett AC; Howard MJ; Mackenzie JS (February 1995). "Immunodominant epitopes on the NS1 protein of MVE and KUN viruses serve as targets for a blocking ELISA to detect virus-specific antibodies in sentinel animal serum". Journal of Virological Methods. 51 (2–3): 201–10. doi:10.1016/0166-0934(94)00105-P. PMID 7738140.
- ↑ California Department of Public Health Tutorial for Local Agencies to Safely Collect Dead Birds Oral Swab Samples on RNAse Cards for West Nile Virus Testing Archived 2014-07-09 at the Wayback Machine.
- ↑ RNA virus preserving filter paper card Archived 2016-01-10 at the Wayback Machine.. fortiusbio.com
- ↑ "Mosquito Monitoring and Management". National Park Service. Archived from the original on 2013-04-15.
- ↑ Oklahoma State University: Mosquitoes and West Nile virus
- ↑ Benedict MQ, Levine RS, Hawley WA, Lounibos LP (2007). "Spread of the tiger: global risk of invasion by the mosquito Aedes albopictus". Vector-Borne and Zoonotic Diseases. 7 (1): 76–85. doi:10.1089/vbz.2006.0562. PMC 2212601. PMID 17417960.
- ↑ Watson JT, Pertel PE, Jones RC, et al. (September 2004). "Clinical characteristics and functional outcomes of West Nile Fever". Ann. Intern. Med. 141 (5): 360–5. doi:10.7326/0003-4819-141-5-200409070-00010. PMID 15353427.
- ↑ Klee AL, Maidin B, Edwin B, et al. (Aug 2004). "Long-term prognosis for clinical West Nile virus infection". Emerg Infect Dis. 10 (8): 1405–11. doi:10.3201/eid1008.030879. PMC 3320418. PMID 15496241.
- ↑ Nolan MS, Podoll AS, Hause AM, Akers KM, Finkel KW, Murray KO (2012). Wang, Tian, ed. "Prevalence of chronic kidney disease and progression of disease over time among patients enrolled in the Houston West Nile virus cohort". PLoS ONE. 7 (7): e40374. doi:10.1371/journal.pone.0040374. PMC 3391259. PMID 22792293.
- ↑ "New Study Reveals: West Nile virus is far more menacing & harms far more people". The Guardian Express. The Guardian Express. 26 August 2012. Archived from the original on 6 October 2012. Retrieved 26 August 2012.
- ↑ Smithburn KC, Hughes TP, Burke AW, Paul JH (June 1940). "A Neurotropic Virus Isolated from the Blood of a Native of Uganda". Am. J. Trop. Med. 20 (1): 471–92.
- ↑ Work TH, Hurlbut HS, Taylor RM (1953). "Isolation of West Nile virus from hooded crow and rock pigeon in the Nile delta". Proc. Soc. Exp. Biol. Med. 84 (3): 719–22. doi:10.3181/00379727-84-20764. PMID 13134268.
- ↑ Bernkopf H, Levine S, Nerson R (1953). "Isolation of West Nile virus in Israel". J. Infect. Dis. 93 (3): 207–18. doi:10.1093/infdis/93.3.207. PMID 13109233.
- ↑ Nash D, Mostashari F, Fine A, et al. (June 2001). "The outbreak of West Nile virus infection in the New York City area in 1999". N. Engl. J. Med. 344 (24): 1807–14. doi:10.1056/NEJM200106143442401. PMID 11407341.
- ↑ Calisher CH (2000). "West Nile virus in the New World: appearance, persistence, and adaptation to a new econiche—an opportunity taken". Viral Immunol. 13 (4): 411–4. doi:10.1089/vim.2000.13.411. PMID 11192287.
- ↑ "West Nile virus". NIOSH. August 27, 2012. Archived from the original on July 29, 2017.
- ↑ Murray KO, Ruktanonchai D, Hesalroad D, Fonken E, Nolan MS (November 2013). "West Nile virus, Texas, USA, 2012". Emerging Infectious Diseases. 19 (11): 1836–8. doi:10.3201/eid1911.130768. PMC 3837649. PMID 24210089. Retrieved 2014-12-08.
- ↑ Fox, M. (May 13, 2013). "2012 was deadliest year for West Nile in US, CDC says". NBC News. Archived from the original on June 8, 2013. Retrieved May 13, 2013.
- ↑ "Vertebrate Ecology". West Nile Virus. Division of Vector-Borne Diseases, CDC. 30 April 2009. Archived from the original on 1 March 2013.
- ↑ Deas, Tia S; Bennett CJ; Jones SA; Tilgner M; Ren P; Behr MJ; Stein DA; Iversen PL; Kramer LD; Bernard KA; Shi PY (May 2007). "In vitro resistance selection and in vivo efficacy of morpholino oligomers against West Nile virus". Antimicrob Agents Chemother. 51 (7): 2470–82. doi:10.1128/AAC.00069-07. PMC 1913242. PMID 17485503.
- ↑ Hayes EB, Sejvar JJ, Zaki SR, Lanciotti RS, Bode AV, Campbell GL (2005). "Virology, pathology, and clinical manifestations of West Nile virus disease". Emerging Infect. Dis. 11 (8): 1174–9. doi:10.3201/eid1108.050289b. PMC 3320472. PMID 16102303. Archived from the original on 2011-08-04.
- ↑ Moskowitz DW, Johnson FE (2004). "The central role of angiotensin I-converting enzyme in vertebrate pathophysiology". Curr Top Med Chem. 4 (13): 1433–54. doi:10.2174/1568026043387818. PMID 15379656.
- ↑ Arroyo, J.; Miller, C.; Catalan, J.; Myers, G. A.; Ratterree, M. S.; Trent, D. W.; Monath, T. P. (2004). "ChimeriVax-West Nile Virus Live-Attenuated Vaccine: Preclinical Evaluation of Safety, Immunogenicity, and Efficacy". Journal of Virology. 78 (22): 12497–12507. doi:10.1128/JVI.78.22.12497-12507.2004. PMC 525070. PMID 15507637.
- ↑ Biedenbender, R.; Bevilacqua, J.; Gregg, A. M.; Watson, M.; Dayan, G. (2011). "Phase II, Randomized, Double-Blind, Placebo-Controlled, Multicenter Study to Investigate the Immunogenicity and Safety of a West Nile Virus Vaccine in Healthy Adults". Journal of Infectious Diseases. 203 (1): 75–84. doi:10.1093/infdis/jiq003. PMC 3086439. PMID 21148499.
External links
| Classification | |
|---|---|
| External resources |
| Wikimedia Commons has media related to West Nile virus. |
- De Filette M, Ulbert S, Diamond M, Sanders NN (2012). "Recent progress in West Nile virus diagnosis and vaccination". Vet. Res. 43 (1): 16. doi:10.1186/1297-9716-43-16. PMC 3311072. PMID 22380523.
- "West Nile Virus". Division of Vector-Borne Diseases, U.S. Centers for Disease Control and Prevention (CDC).
- CDC—West Nile Virus—NIOSH Workplace Safety and Health Topic
- West Nile Virus Resource Guide—National Pesticide Information Center
- Vaccine Research Center (VRC)—Information concerning WNV vaccine research studies
- Virus Pathogen Database and Analysis Resource (ViPR): Flaviviridae
- Species Profile- West Nile Virus (Flavivirus), National Invasive Species Information Center, United States National Agricultural Library. Lists general information and resources for West Nile Virus.
- West Nile Virus—West Nile Encephalitis Brain Scans