Atrioventricular block
| Atrioventricular block | |
|---|---|
| Classification and external resources | |
| Specialty | cardiology |
| ICD-10 | I44.0-I44.3 |
| ICD-9-CM | 426.0-426.1 |
| eMedicine | med/189 |
| MeSH | D054537 |
Atrioventricular block (AV block) is a type of heart block in which the conduction between the atria and ventricles of the heart is impaired. Under normal conditions, the sinoatrial node (SA node) in the atria sets the pace for the heart, and these impulses travel down to the ventricles. In an AV block, this message does not reach the ventricles or is impaired along the way. The ventricles of the heart have their own pacing mechanisms, which can maintain a lowered heart rate in the absence of SA stimulation.
The causes of pathological AV block are varied and include ischaemia, infarction, fibrosis or drugs, and the blocks may be complete or may only impair the signaling between the SA and AV nodes. Certain AV blocks can also be found as normal variants, such as in athletes or children, and are benign.[1] Strong vagal stimulation may also produce AV block. The cholinergic receptor types affected are the muscarinic receptors.
There are three types:
- First-degree atrioventricular block - The heart’s electrical signals move between the upper and lower chambers of the heart.[2]PR interval greater than 0.20sec.
- Second-degree atrioventricular block - The heart’s electrical signals between the upper and lower signals of the heart are slowed by a much greater rate than in first-degree atrioventricular block.[2] Type 1 (a.k.a. Mobitz 1, Wenckebach): Progressive prolongation of PR interval with dropped beats (the PR interval gets longer and longer; finally one beat drops) . Type 2 (a.k.a. Mobitz 2, Hay): PR interval remains unchanged prior to the P wave which suddenly fails to conduct to the ventricles.
- Mobitz I is characterized by a reversible block of the AV node. When the AV node is severely blocked, it fails to conduct an impulse. Mobitz I is a progressive failure. Some patients are asymptomatic; those who have symptoms respond to treatment effectively. There is low risk of the AV block leading to heart attack.
- Mobitz II is characterized by a failure of the His-Purkinje cells resulting in the lack of a supra ventricular impulse. These cardiac His-Purkinje cells are responsible for the rapid propagation in the heart. Mobitz II is caused by a sudden and unexpected failure of the His-Purkinje cells. The risks and possible effects of Mobitz II are much more severe than Mobitz I in that it can lead to severe heart attack.[3]
- Third-degree atrioventricular block - No association between P waves and QRS complexes. The heart’s electrical signals are slowed to a complete halt. This means that none of the signals reach either the upper or lower chambers causing a complete blockage of the ventricles and can result in cardiac arrest. Third-degree atrioventricular block is the most severe of the types of heart ventricle blockages. Persons suffering from symptoms of third-degree heart block need emergency treatment including but not limited to a pacemaker.[2]
In order to differentiate between the different degrees of the atrioventricular block (AV block), the First-Degree AV block occurs when an electrocardiogram (ECG) reads a PR interval that is more than 200 msec. This degree is typically asymptomatic and is only found through an ECG reading. Second-Degree AV block, although typically asymptomatic, has early signs that can be detected or are noticeable such as irregular heartbeat or a syncope. A Third-Degree AV block, has noticeable symptoms that present itself as more urgent such as: dizziness, fatigue, chest pain, pre syncope, or syncope.[4]
Laboratory diagnosis for AV blocks include electrolyte, drug level and cardiac enzyme level tests. A clinical evaluation also looks at infection, myxedema, or connective tissue disease studies. In order to properly diagnose a patient with AV block, an electrocardiographic recording must be completed (ECG). Based on the P waves and QRS complexes that can be evaluated from these readings, that relationship will be the standardized test if an AV block is present or not. In order to identify this block based on the readings the following must occur: multiple ECG recordings, 24-hour Holter monitoring, and implant loop recordings. Other examinations for the detection of an AV block include electrophysiologic testing, echocardiography, and exercise.[4]
Management includes a form of pharmacologic therapy that administers anticholinergic agents and is dependent upon the severity of a blockage. In severe cases or emergencies, atropine administration or isoproterenol infusion would allow for temporary relief if bradycardia is the cause for the blockage, but if His-Purkinje system is the result of the AV block then pharmacologic therapy is not recommended.[4]
 Sinus rhythm with acute inferior infarction complicated by Type I A-V block manifest in the form of 5:4 Wenckebach periods; R-P/P-R reciprocity.
Sinus rhythm with acute inferior infarction complicated by Type I A-V block manifest in the form of 5:4 Wenckebach periods; R-P/P-R reciprocity.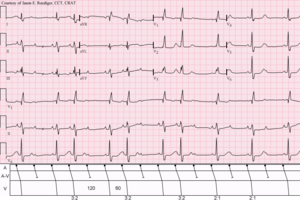 Sinus rhythm (rate = 100/min) with 3:2 and 2:1 Type II A-V block; RBBB
Sinus rhythm (rate = 100/min) with 3:2 and 2:1 Type II A-V block; RBBB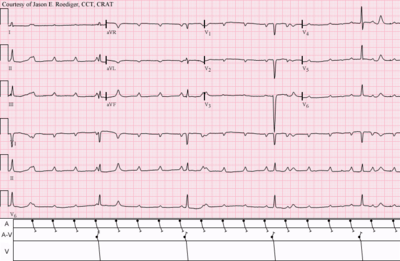 Sinus tachycardia with complete A-V block and resulting junctional escape
Sinus tachycardia with complete A-V block and resulting junctional escape
References
- ↑ Lilly, Leonard (2006). Pathophysiology of Heart Disease. Lippincott Williams & Wilkins. ISBN 978-0-7817-6321-9.
- 1 2 3 "Types of Heart Block - NHLBI, NIH". www.nhlbi.nih.gov. Retrieved 2017-03-22.
- ↑ Wogan, J. M.; Lowenstein, S. R.; Gordon, G. S. (1993-01-01). "Second-degree atrioventricular block: Mobitz type II". The Journal of Emergency Medicine. 11 (1): 47–54. doi:10.1016/0736-4679(93)90009-v. ISSN 0736-4679. PMID 8445186.
- 1 2 3 "Atrioventricular Block: Practice Essentials, Background, Pathophysiology". 2017-01-06.