Lymph node
| Lymph node | |
|---|---|
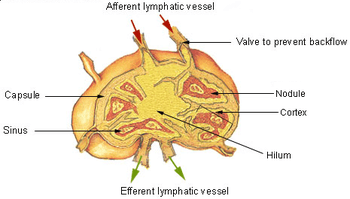
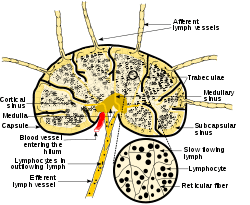 Diagram of a lymph node, showing the flow of lymph through the lymph sinuses. | |
| Details | |
| System | Immune system[1][2] (Lymphatic system) |
| Identifiers | |
| Latin | nodus lymphaticus (singular); nodi lymphatici (plural) |
| MeSH | D008198 |
| TA | A13.2.03.001 |
| FMA | 5034 |
| Anatomical terminology | |
A lymph node or lymph gland is an ovoid or kidney-shaped organ of the lymphatic system, and of the adaptive immune system, that is widely present throughout the body. They are linked by the lymphatic vessels as a part of the circulatory system. Lymph nodes are major sites of B and T lymphocytes, and other white blood cells. Lymph nodes are important for the proper functioning of the immune system, acting as filters for foreign particles and cancer cells. Lymph nodes do not have a detoxification function, which is primarily dealt with by the liver and kidneys.
In the lymphatic system the lymph node is a secondary lymphoid organ.[3] A lymph node is enclosed in a fibrous capsule and is made up of an outer cortex and an inner medulla.[3]
Lymph nodes also have clinical significance. They become inflamed or enlarged in various diseases which may range from trivial throat infections, to life-threatening cancers. The condition of the lymph nodes is very important in cancer staging, which decides the treatment to be used, and determines the prognosis. When swollen, inflamed or enlarged, lymph nodes can be hard, firm or tender.[4]
Structure
.jpg)
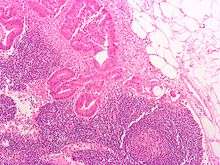
Lymph nodes are kidney or oval shaped and range in size from a few millimeters to about 1–2 cm long.[5] Each lymph node is surrounded by a fibrous capsule, which extends inside the lymph node to form trabeculae. The substance of the lymph node is divided into the outer cortex and the inner medulla. The cortex is continuous around the medulla except where the medulla comes into direct contact with the hilum.[5]
Thin reticular fibers of reticular connective tissue, and elastin form a supporting meshwork called a reticulin inside the node. B cells are mainly found in the outer (superficial) cortex where they are clustered together as follicular B cells in lymphoid follicles and the T cells are mainly in the paracortex.[6] The lymph node is divided into compartments called lymph nodules (or lobules) each consisting of a cortical region of combined follicle B cells, a paracortical region of T cells, and a basal part of the nodule in the medulla.[7]
The number and composition of follicles can change especially when challenged by an antigen, when they develop a germinal center.[5] Elsewhere in the node, there are only occasional leukocytes. As part of the reticular network there are follicular dendritic cells in the B cell follicle and fibroblastic reticular cells in the T cell cortex. The reticular network not only provides the structural support, but also the surface for adhesion of the dendritic cells, macrophages and lymphocytes. It allows exchange of material with blood through the high endothelial venules and provides the growth and regulatory factors necessary for activation and maturation of immune cells.[8]
Lymph enters the convex side of the lymph node through multiple afferent lymphatic vessels, and flows through spaces called sinuses. A lymph sinus which includes the subcapsular sinus, is a channel within the node, lined by endothelial cells along with fibroblastic reticular cells and this allows for the smooth flow of lymph through them.The endothelium of the subcapsular sinus is continuous with that of the afferent lymph vessel and is also with that of the similar sinuses flanking the trabeculae and within the cortex. All of these sinuses drain the filtered lymphatic fluid into the medullary sinuses, from where the lymph flows into the efferent lymph vessels to exit the node at the hilum on the concave side.[5] These vessels are smaller and don't allow the passage of the macrophages so that they remain contained to function within the lymph node. In the course of the lymph, lymphocytes may be activated as part of the adaptive immune response.
Capsule
The lymph node capsule is composed of dense irregular connective tissue with some plain collagenous fibers, and from its internal surface are given off a number of membranous processes or trabeculae. They pass inward, radiating toward the center of the node, for about one-third or one-fourth of the space between the circumference and the center of the node. In some animals they are sufficiently well-marked to divide the peripheral or cortical portion of the node into a number of compartments (nodules), but in humans this arrangement is not obvious. The larger trabeculae springing from the capsule break up into finer bands, and these interlace to form a mesh-work in the central or medullary portion of the node. In these trabecular spaces formed by the interlacing trabeculae is contained the proper lymph node substance or lymphoid tissue. The node pulp does not, however, completely fill the spaces, but leaves, between its outer margin and the enclosing trabeculae, a channel or space of uniform width throughout. This is termed the subcapsular sinus (lymph path or lymph sinus). Running across it are a number of finer trabeculae of reticular connective tissue, the fibers of which are, for the most part, covered by ramifying cells.
Subcapsular sinus
The subcapsular sinus (lymph path, lymph sinus, marginal sinus) is the space between the capsule and the cortex which allows the free movement of lymphatic fluid and so contains few lymphocytes.[5] It is continuous with the similar lymph sinuses that flank the trabeculae.[5]
The lymph node contains lymphoid tissue, i.e., a meshwork or fibers called reticulum with white blood cells enmeshed in it. The regions where there are few cells within the meshwork are known as lymph sinus. It is lined by reticular cells, fibroblasts and fixed macrophages.[5]
The subcapsular sinus has clinical importance as it is the most likely location where the earliest manifestations of a metastatic carcinoma in a lymph node would be found.
Cortex

The cortex of the lymph node is the outer portion of the node, underneath the capsule and the subcapsular sinus.[7] It has an outer superficial part and a deeper part known as the paracortex.[7] The subcapsular sinus drains to the trabecular sinuses, and then the lymph flows into the medullary sinuses.
The outer cortex consists mainly of the B cells arranged as follicles, which may develop a germinal center when challenged with an antigen, and the deeper paracortex mainly consists of the T cells. Here the T-cells mainly interact with dendritic cells, and the reticular network is dense.[9]
Medulla
The medulla contains large blood vessels, sinuses and medullary cords that contain antibody-secreting plasma cells.
The medullary cords are cords of lymphatic tissue, and include plasma cells, macrophages, and B cells. The medullary sinuses (or sinusoids) are vessel-like spaces separating the medullary cords. Lymph flows into the medullary sinuses from cortical sinuses, and into the efferent lymphatic vessel. There is usually only one efferent vessel though sometimes there may be two.[10] Medullary sinuses contain histiocytes (immobile macrophages) and reticular cells.
Location
Lymph nodes are present throughout the body, are more concentrated near and within the trunk, and are divided in the study of anatomy into groups. Some lymph nodes can be felt when enlarged (and occasionally when not), such as the axillary lymph nodes under the arm, the cervical lymph nodes of the head and neck and the inguinal lymph nodes near the groin crease. Some lymph nodes can be seen, such as the tonsils. Most lymph nodes however lie within the trunk adjacent to other major structures in the body - such as the paraaortic lymph nodes and the tracheobronchial lymph nodes.
There are no lymph nodes in the central nervous system, which is separated from the body by the blood-brain barrier.
Function
The primary function of lymph nodes is the filtering of lymph to identify and fight infection. In order to do this, lymph nodes contain lymphocytes, a type of white blood cell, which includes B cells and T cells. These circulate through the bloodstream and enter and reside in lymph nodes.[11] B cells produce antibodies. Each antibody has a single predetermined target, an antigen, that it can bind to. These circulate throughout the bloodstream and if they find this target, the antibodies bind to it and stimulate an immune response. Each B cell produces different antibodies, and this process is driven in lymph nodes. B cells enter the bloodstream as "naive" cells produced in bone marrow. After entering a lymph node, they then enter a lymphoid follicle, where they multiply and divide, each producing a different antibody. If a cell is stimulated, it will go on to produce more antibodies (a plasma cell) or act as a memory cell to help the body fight future infection.[12] If a cell is not stimulated, it will undergo apoptosis and die.[12]
Antigens are molecules found on bacterial cell walls, chemical substances secreted from bacteria, or sometimes even molecules present in body tissue itself. These are taken up by cells throughout the body called antigen-presenting cells, such as dendritic cells.[13] These antigen presenting cells enter the lymph system and then lymph nodes. They present the antigen to T cells and, if there is a T cell with the appropriate T cell receptor, it will be activated.[12]
B cells acquire antigen directly from the afferent lymph. If a B cell binds its cognate antigen it will be activated. Some B cells will immediately develop into antibody secreting plasma cells, and secrete IgM. Other B cells will internalize the antigen and present it to Follicular helper T cells on the B and T cell zone interface. If a cognate FTh cell is found it will upregulate CD40L and promote somatic hypermutation and isotype class switching of the B cell, increasing its antigen binding affinity and changing its effector function. Proliferation of cells within the lymph node will make the node expand.
Lymph is present throughout the body, and circulates through lymphatic vessels. These drain into and from lymph nodes – afferent vessels drain into nodes, and efferent vessels from nodes. When lymph fluid enters a node, it drains into the node just beneath the capsule in a space called the subcapsular sinus. The subcapsular sinus drains into trabecular sinuses and finally into medullary sinuses. The sinus space is criss-crossed by the pseudopods of macrophages, which act to trap foreign particles and filter the lymph. The medullary sinuses converge at the hilum and lymph then leaves the lymph node via the efferent lymphatic vessel towards either a more central lymph node or ultimately for drainage into a central venous subclavian blood vessel.
- The B cells migrate to the nodular cortex and medulla.
- The T cells migrate to the deep cortex. This is a region of the lymph node called the paracortex that immediately surrounds the medulla. Unlike the cortex, which has mostly immature T cells, or thymocytes, the paracortex has a mixture of immature and mature T cells. Lymphocytes enter the lymph nodes through specialized high endothelial venules found in the paracortex.
The spleen and tonsils are the larger secondary lymphoid organs that serve similar functions to lymph nodes, though the spleen filters blood cells rather than lymph.
Clinical significance
Swelling
Lymph nodes may become enlarged due to an infection, tumor, autoimmune disease, drug reactions, or to leukemia.[14] Swollen lymph nodes (or the disease causing them) are referred to as lymphadenopathy.[15] Swollen lymph nodes may be seen, as in enlarged tonsils, or seen as gross enlargement of nodes due to lymphoma. They may be felt, or seen on a scan. Swollen lymph nodes may be painful or cause other symptoms such as a difficulty in swallowing or in breathing. When very large they may compress on a blood vessel. Swelling can occur in one node, in a localised area, or be widespread.
The taking of a medical history and exam by a medical practitioner can help point to the cause of the swelling, whether it be a localised infection, or a systemic disorder. Many symptoms or signs may point to the cause of swelling - for example, a sore throat and a cough may point to an upper respiratory tract infection as the cause of tonsil swelling. Changes in the appearance of a breast or a mass that has been felt may explain underarm pain and axillary lymph node swelling. Ongoing fevers or night sweats may suggest a systemic infection or a lymphoma as the cause of swelling. Depending on these findings, a wide variety of medical tests that include blood tests and scans may be needed to further examine the cause. A biopsy of a lymph node may also be needed.
Lymphedema is another and fairly widespread condition that results in fluid retention and tissue swelling. It can be congenital as a result usually of undeveloped or absent lymph nodes, and is known as primary lymphedema. Secondary lymphedema usually results from the removal of lymph nodes during breast cancer surgery or from other damaging treatments such as radiation. It can also be caused by some parasitic infections. Affected tissues are at a great risk of infection.
Cancer
Lymph nodes can be affected by both primary cancers of lymph tissue, and secondary cancers affecting other part of the body. Primary cancers of lymph tissue are called lymphomas and include Hodgkin lymphoma and non-Hodgkin lymphoma. Cancer of lymph nodes can cause a wide range of symptoms from painless long-term slowly growing swelling to sudden, rapid enlargement over days or weeks. Lymphoma is managed by haematologists and oncologists
Local cancer in many parts of the body can cause lymph nodes to enlarge, usually because of tumours cells that have metastasised into the node. Lymph node involvement is often a key part in the diagnosis and treatment of cancer, acting as "sentinels" of local disease, incorporated into TNM staging and other cancer staging systems. As part of the investigations or workup for cancer, lymph nodes may be imaged or even surgically removed. Whether lymph nodes are affected will affect the stage of the cancer and overall treatment and prognosis.
Additional images
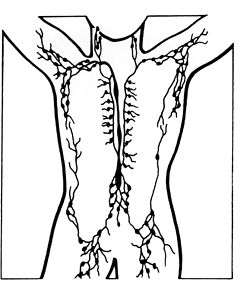
 Lymphatic system
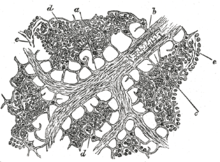
Lymphatic system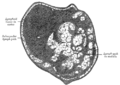 Section of small lymph node of rabbit.
Section of small lymph node of rabbit.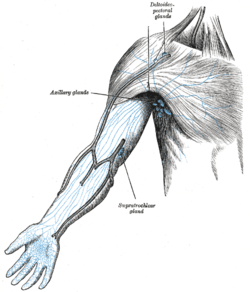 Lymphatics of the arm
Lymphatics of the arm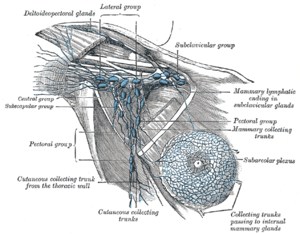 Lymphatics of the axillary region
Lymphatics of the axillary region Lymph node histology
Lymph node histology
See also
- Peyer's patch
- Kawasaki disease - Lymph node syndrome
- Bubonic plague
References
- ↑ "What are lymph nodes". Siamak N. Nabili, MD, MPH. 2015-02-05.
- ↑ "Lymph Nodes Directory". www.webmd.com.
- 1 2 Pocock, Gillian; Richards, Christopher D. (2006). Human physiology : the basis of medicine (3rd ed.). Oxford: Oxford University Press. pp. 252–253. ISBN 978-0-19-856878-0.
- ↑ "Swollen Glands and Other Lumps Under the Skin-Topic Overview". Children.webmd.com. 2011-04-14. Retrieved 2014-02-28.
- 1 2 3 4 5 6 7 Warwick, Roger; Peter L. Williams (1973) [1858]. "Angiology (Chapter 6)". Gray's anatomy. illustrated by Richard E. M. Moore (Thirty-fifth ed.). London: Longman. pp. 588–785.
|access-date=requires|url=(help) - ↑ Alberts, Bruce (1994). Molecular biology of the cell (3rd ed.). New York, N.Y.: Garland STPM. p. 1202. ISBN 0-8153-1620-8.
- 1 2 3 Willard-Mack, Cynthia L. (25 June 2016). "Normal Structure, Function, and Histology of Lymph Nodes". Toxicologic Pathology. doi:10.1080/01926230600867727#_i15%20_i16.
- ↑ Kaldjian, Eric P.; J. Elizabeth Gretz; Arthur O. Anderson; Yinghui Shi; Stephen Shaw (October 2001). "Spatial and molecular organization of lymph node T cell cortex: a labyrinthine cavity bounded by an epithelium-like monolayer of fibroblastic reticular cells anchored to basement membrane-like extracellular matrix". International Immunology. Oxford Journals. 13 (10): 1243–1253. doi:10.1093/intimm/13.10.1243. PMID 11581169. Retrieved 2008-07-11.
- ↑ Katakai, Tomoya; Takahiro Hara; Hiroyuki Gonda; Manabu Sugai; Akira Shimizu (5 July 2004). "A novel reticular stromal structure in lymph node cortex: an immuno-platform for interactions among dendritic cells, T cells and B cells". International Immunology. 16 (8): 1133–1142. doi:10.1093/intimm/dxh113. PMID 15237106. Retrieved 2008-07-11.
- ↑ Henrikson, Ray C.; Mazurkiewicz, Joseph E. (1 January 1997). "Histology". Lippincott Williams & Wilkins.
- ↑ Hoffbrand's 2016, p. 103,110.
- 1 2 3 Hoffbrand's 2016, p. 111.
- ↑ Hoffbrand's 2016, p. 109.
- ↑ Hoffbrand's 2016, p. 114.
- ↑ Choices, NHS. "Swollen glands - NHS Choices". www.nhs.uk.
- Books
- Britton, the editors Nicki R. Colledge, Brian R. Walker, Stuart H. Ralston ; illustrated by Robert (2010). Davidson's principles and practice of medicine (21st ed.). Edinburgh: Churchill Livingstone/Elsevier. ISBN 978-0-7020-3085-7.
- Deakin, Barbara Young ... [et al.] ; drawings by Philip J. (2006). Wheater's functional histology : a text and colour atlas (5th ed.). [Edinburgh?]: Churchill Livingstone/Elsevier. ISBN 9780443068508.
- Hoffbrand, Victor; Moss, Paul A. H. (2016). Hoffbrand's essential haematology (7th ed.). West Sussex: Wiley Blackwell. ISBN 978-1-1184-0867-4.
External links
| Wikimedia Commons has media related to Lymph nodes. |
- Histology image: 07101loa – Histology Learning System at Boston University
- Lymph Nodes
- Lymph Nodes Drainage
Human systems and organs | |||||||
|---|---|---|---|---|---|---|---|
| Musculoskeletal |
| ||||||
| Circulatory system |
| ||||||
| Nervous system | |||||||
| Integumentary system | |||||||
| Immune system | |||||||
| Respiratory system | |||||||
| Digestive system | |||||||
| Urinary system | |||||||
| Reproductive system | |||||||
| Endocrine system | |||||||
| |||||||