Spanish flu
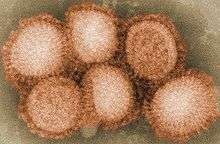
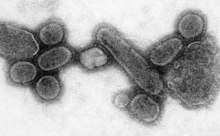
The Spanish flu, also known as the 1918 flu pandemic, was an unusually deadly influenza pandemic caused by the H1N1 influenza A virus. Lasting February 1918 to April 1920, it infected 500 million people–about a third of the world's population at the time–in four successive waves. The death toll may have been anything from 17 million to 50 million, and possibly as high as 100 million, making it one of the deadliest pandemics in human history.[3]
| Spanish flu | |
|---|---|
 | |
| Disease | Influenza |
| Virus strain | Strains of A/H1N1 |
| Location | Worldwide |
| First outbreak | Disputed |
| Date | February 1918 – April 1920[1] |
| Suspected cases‡ | 500 million (estimate)[2] |
Deaths | 17–50+ million (estimate) |
| ‡Suspected cases have not been confirmed as being due to this strain by laboratory tests, although some other strains may have been ruled out. | |
| Influenza (Flu) |
|---|
 |
|
The first observations of illness and mortality were documented in the United States (in Fort Riley, Haskell County, Kansas as well as in New York City), France (Brest), Germany and the United Kingdom. To maintain morale, World War I censors minimized these early reports. Newspapers were free to report the epidemic's effects in neutral Spain, such as the grave illness of King Alfonso XIII, and these stories created a false impression of Spain as especially hard hit. This gave rise to the name "Spanish" flu. Historical and epidemiological data are inadequate to identify with certainty the pandemic's geographic origin, with varying views as to its location.
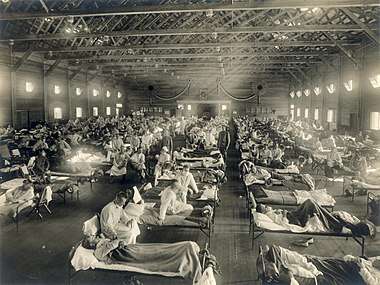
Most influenza outbreaks disproportionately kill the very young and the very old, with a higher survival rate for those in between, but the Spanish flu pandemic resulted in a higher than expected mortality rate for young adults.[4] Scientists offer several possible explanations for the high mortality rate of the 1918 influenza pandemic. Some analyses have shown the virus to be particularly deadly because it triggers a cytokine storm, which ravages the stronger immune system of young adults.[5] In contrast, a 2007 analysis of medical journals from the period of the pandemic found that the viral infection was no more aggressive than previous influenza strains.[6][7] Instead, malnourishment, overcrowded medical camps and hospitals, and poor hygiene, all exacerbated by the recent war, promoted bacterial superinfection. This superinfection killed most of the victims, typically after a somewhat prolonged death bed.[8][9]
The 1918 Spanish flu was the first of two pandemics caused by H1N1 influenza A virus; the second was the 2009 swine flu pandemic.[10]
Etymology
The origin of the "Spanish flu" name stems from the pandemic's spread to Spain from France in November 1918.[11][12] Spain was not involved in the war, having remained neutral, and had not imposed wartime censorship.[13][14] Newspapers were therefore free to report the epidemic's effects, such as the grave illness of King Alfonso XIII, and these widely-spread stories created a false impression of Spain as especially hard hit.[15]
Alternative names were also used at the time of the pandemic. Similar to the name of Spanish flu, many of these also alluded to the purported origins of the disease. In Senegal it was named 'the Brazilian flu', and in Brazil 'the German flu', while in Poland it was known as 'the Bolshevik disease'.[16] In Spain itself, the nickname for the flu, the "Naples Soldier", was adopted from a 1916 operetta, The Song of Forgetting (La canción del olvido) after one of the librettists quipped that the play's most popular musical number, Naples Soldier, was as catchy as the flu.[17]
Nearly a century after the Spanish flu struck in 1918–1920, the World Health Organization (WHO) called on scientists, national authorities and the media to follow best practices in naming new human infectious diseases to minimize unnecessary negative effects on nations, economies and people - this includes a recommendation to no longer name diseases after places.[18][19] More modern terms for this virus include the "1918 influenza pandemic," the "1918 flu pandemic," or variations of these.[20][21][22]
History
Timeline
First wave of early 1918
The pandemic is conventionally marked as having begun on 4 March 1918, with the recording of the case of Albert Gitchell, an army cook at Camp Funston in Kansas, United States, despite there likely having been cases before him.[23] The disease had been observed in Haskell County in January 1918, prompting local doctor Loring Miner to warn the US Public Health Service's academic journal.[24] Within days, 522 men at the camp had reported sick.[25] By 11 March 1918, the virus had reached Queens, New York.[26] Failure to take preventive measures in March/April was later criticised.[27]
As the US had entered World War I, the disease quickly spread from Camp Funston, a major training ground for troops of the American Expeditionary Forces, to other US Army camps and Europe, becoming an epidemic in the Midwest, East Coast, and French ports by April 1918, and reaching the Western Front by the middle of the month.[23] It then quickly spread to the rest of France, Great Britain, Italy, and Spain, and in May reached Wrocław and Odessa.[23] After the signing of the Treaty of Brest-Litovsk, Germany started releasing Russian prisoners of war who then brought the disease to their country.[28] It reached North Africa, India, and Japan in May, and soon after had likely gone around the world as there had been recorded cases in Southeast Asia in April.[29] In June an outbreak was reported in China.[30] After reaching Australia in July, the wave started to recede.[29]
The first wave of the flu lasted from the first quarter of 1918, and was relatively mild.[31] Mortality rates were not appreciably above normal;[32] in the United States ~75,000 flu-related deaths were reported in the first six months of 1918, compared to ~63,000 deaths during the same time period in 1915.[33] In Madrid, Spain, fewer than 1,000 people died from influenza between May and June 1918.[34] There were no reported quarantines during the first quarter of 1918. However, the first wave caused a significant disruption in the military operations of World War I, with three-quarters of French troops, half the British forces, and over 900,000 German soldiers sick.[35]
.jpg)
Deadly second wave of late 1918
The second wave began in the second half of August, probably spreading to Boston and Freetown, Sierra Leone by ships from Brest, where it had likely arrived with American troops or French recruits for naval training.[35] From the Boston Navy Yard and Camp Devens (later renamed Fort Devens), about 30 miles west of Boston, other U.S. military sites were soon afflicted, as were troops being transported to Europe.[36] Helped by troop movements, it spread over the next two months to all of North America, and then to Central and South America, also reaching Brazil and the Caribbean on ships.[37] From Freetown, the pandemic continued to spread through West Africa along the coast, rivers, and the colonial railways, and from railheads to more remote communities, while South Africa received it in September on ships bringing back members of the South African Native Labour Corps returning from France.[37] From there it spread around Southern Africa and beyond the Zambezi, reaching Ethiopia in November.[38]
From Europe the second wave swept through Russia in a southwest-northeast diagonal front, as well as being brought to Arkhangelsk by the North Russia intervention, and then spread throughout Asia following the Russian Civil War and the Trans-Siberian railway, reaching Iran (where it spread through the holy city of Mashhad), and then later India in September, as well as China and Japan in October.[39] The celebrations of the Armistice of 11 November 1918 also caused outbreaks in Lima and Nairobi, but by December the wave was mostly over.[40]

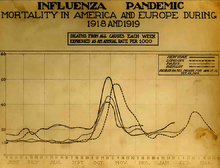
The second wave of the 1918 pandemic was much more deadly than the first. The first wave had resembled typical flu epidemics; those most at risk were the sick and elderly, while younger, healthier people recovered easily. October 1918 was the month with the highest fatality rate of the whole pandemic.[41]
Third wave of 1919
In January 1919 a third wave of the Spanish Flu hit Australia, where it killed 12,000 following the lifting of a maritime quarantine, and then spread quickly through Europe and the United States, where it lingered through the Spring and until June 1919.[42][43][44][40] It primarily affected Spain, Serbia, Mexico and Great Britain, resulting in hundreds of thousands of deaths.[45] It was less severe than the second wave but still much more deadly than the initial first wave. In the United States, isolated outbreaks occurred in some cities including Los Angeles,[46] New York City,[47] Memphis, Nashville, San Francisco and St. Louis.[48] Overall American mortality rates were in the tens of thousands during the first six months of 1919.[49]
Fourth wave of 1920
In spring 1920 a very minor fourth wave occurred in isolated areas including New York City,[47] the United Kingdom, Austria, Scandinavia, and some South American islands.[50] Peru experienced a late wave in early 1920, and Japan had one from late 1919 to 1920, with the last cases in March.[51]

Potential origins
Despite its name, historical and epidemiological data cannot identify the geographic origin of the Spanish flu.[2] However, several theories have been proposed.
United States
The first confirmed cases originated in the United States. Historian Alfred W. Crosby stated in 2003 that the flu originated in Kansas,[52] and popular author John M. Barry described a January 1918 outbreak in Haskell County, Kansas, as the point of origin in his 2004 article.[5]
A 2018 study of tissue slides and medical reports led by evolutionary biology professor Michael Worobey found evidence against the disease originating from Kansas, as those cases were milder and had fewer deaths compared to the infections in New York City in the same time period. The study did find evidence through phylogenetic analyses that the virus likely had a North American origin, though it was not conclusive. In addition, the haemagglutinin glycoproteins of the virus suggest that it originated long before 1918, and other studies suggest that the reassortment of the H1N1 virus likely occurred in or around 1915.[53]
Europe
The major UK troop staging and hospital camp in Étaples in France has been theorized by virologist John Oxford as being at the center of the Spanish flu.[54] His study found that in late 1916 the Étaples camp was hit by the onset of a new disease with high mortality that caused symptoms similar to the flu.[55][54] According to Oxford, a similar outbreak occurred in March 1917 at army barracks in Aldershot,[56] and military pathologists later recognized these early outbreaks as the same disease as the 1918 flu.[57][54] The overcrowded camp and hospital was an ideal environment for the spread of a respiratory virus. The hospital treated thousands of victims of poison gas attacks, and other casualties of war, and 100,000 soldiers passed through the camp every day. It also was home to a piggery, and poultry was regularly brought in from surrounding villages to feed the camp. Oxford and his team postulated that a precursor virus, harbored in birds, mutated and then migrated to pigs kept near the front.[56][57]
A report published in 2016 in the Journal of the Chinese Medical Association found evidence that the 1918 virus had been circulating in the European armies for months and possibly years before the 1918 pandemic.[58] Political scientist Andrew Price-Smith published data from the Austrian archives suggesting the influenza began in Austria in early 1917.[59]
China
In 1993, Claude Hannoun, the leading expert on the 1918 flu at the Pasteur Institute, asserted the precursor virus was likely to have come from China and then mutated in the United States near Boston and from there spread to Brest, France, Europe's battlefields, the rest of Europe, and the rest of the world, with Allied soldiers and sailors as the main disseminators.[60] Hannoun considered several alternative hypotheses of origin, such as Spain, Kansas, and Brest, as being possible, but not likely.[60] In 2014, historian Mark Humphries argued that the mobilization of 96,000 Chinese laborers to work behind the British and French lines might have been the source of the pandemic. Humphries, of the Memorial University of Newfoundland in St. John's, based his conclusions on newly unearthed records. He found archival evidence that a respiratory illness that struck northern China (where the laborers came from) in November 1917 was identified a year later by Chinese health officials as identical to the Spanish flu.[61][62] However, no tissue samples have survived for modern comparison.[63] Nevertheless, there were some reports of respiratory illness on parts of the path the laborers took to get to Europe, which also passed through North America.[63]
One of the few regions of the world seemingly less affected by the 1918 flu pandemic was China, where several studies have documented a comparatively mild flu season in 1918.[64][65][66] (Although this is disputed due to lack of data during the Warlord Period, see Around the globe). This has led to speculation that the 1918 flu pandemic originated in China,[66][65][67][68] as the lower rates of flu mortality may be explained by the Chinese population's previously acquired immunity to the flu virus.[69][66][65]
A report published in 2016 in the Journal of the Chinese Medical Association found no evidence that the 1918 virus was imported to Europe via Chinese and Southeast Asian soldiers and workers and instead found evidence of its circulation in Europe before the pandemic.[58] The 2016 study suggested that the low flu mortality rate (an estimated one in a thousand) found among the Chinese and Southeast Asian workers in Europe meant that the deadly 1918 influenza pandemic could not have originated from those workers.[58] Further evidence against the disease being spread by Chinese workers was that workers entered Europe through other routes that did not result in a detectable spread, making them unlikely to have been the original hosts.[53]
Epidemiology and pathology
Transmission and mutation

The basic reproduction number of the virus was between 2 and 3.[70] The close quarters and massive troop movements of World War I hastened the pandemic, and probably both increased transmission and augmented mutation. The war may also have reduced people's resistance to the virus. Some speculate the soldiers' immune systems were weakened by malnourishment, as well as the stresses of combat and chemical attacks, increasing their susceptibility.[71][72] A large factor in the worldwide occurrence of the flu was increased travel. Modern transportation systems made it easier for soldiers, sailors, and civilian travelers to spread the disease.[26] Another was lies and denial by governments, leaving the population ill-prepared to handle the outbreaks.[73]
The severity of the second wave has been attributed to the circumstances of the First World War.[74] In civilian life, natural selection favors a mild strain. Those who get very ill stay home, and those mildly ill continue with their lives, preferentially spreading the mild strain. In the trenches, natural selection was reversed. Soldiers with a mild strain stayed where they were, while the severely ill were sent on crowded trains to crowded field hospitals, spreading the deadlier virus. The second wave began, and the flu quickly spread around the world again. Consequently, during modern pandemics, health officials pay attention when the virus reaches places with social upheaval (looking for deadlier strains of the virus).[75] The fact that most of those who recovered from first-wave infections had become immune showed that it must have been the same strain of flu. This was most dramatically illustrated in Copenhagen, which escaped with a combined mortality rate of just 0.29% (0.02% in the first wave and 0.27% in the second wave) because of exposure to the less-lethal first wave.[76] For the rest of the population, the second wave was far more deadly; the most vulnerable people were those like the soldiers in the trenches – adults who were young and fit.[77]
After the lethal second wave struck in late 1918, new cases dropped abruptly – almost to nothing after the peak in the second wave.[78] In Philadelphia, for example, 4,597 people died in the week ending 16 October, but by 11 November, influenza had almost disappeared from the city. One explanation for the rapid decline in the lethality of the disease is that doctors became more effective in prevention and treatment of the pneumonia that developed after the victims had contracted the virus. However, John Barry stated in his 2004 book The Great Influenza: The Epic Story of the Deadliest Plague In History that researchers have found no evidence to support this position.[5] Another theory holds that the 1918 virus mutated extremely rapidly to a less lethal strain. This is a common occurrence with influenza viruses: there is a tendency for pathogenic viruses to become less lethal with time, as the hosts of more dangerous strains tend to die out.[5] Some fatal cases did continue into March 1919, killing one player in the 1919 Stanley Cup Finals.
Signs and symptoms

The majority of the infected experienced only the typical flu symptoms of sore throat, headache, and fever, especially during the first wave.[79] However, during the second wave the disease was much more serious, often complicated by bacterial pneumonia, which was often the cause of death.[79] This more serious type would cause heliotrope cyanosis to develop, whereby the skin would first develop two mahogany spots over the cheekbones which would then over a few hours spread to color the entire face blue, followed by black coloration first in the extremities and then further spreading to the limbs and the torso.[79] After this, death would follow within hours or days due to the lungs being filled with fluids.[79] Other signs and symptoms reported included spontaneous mouth and nosebleeds, miscarriages for pregnant women, a peculiar smell, teeth and hair falling, delirium, dizziness, insomnia, loss of hearing or smell, blurred vision, and impaired color vision.[79] One observer wrote, "One of the most striking of the complications was hemorrhage from mucous membranes, especially from the nose, stomach, and intestine. Bleeding from the ears and petechial hemorrhages in the skin also occurred".[80] The severity of the symptoms was believed to be caused by cytokine storms.[81]
The majority of deaths were from bacterial pneumonia,[82][83][84] a common secondary infection associated with influenza. This pneumonia was itself caused by common upper respiratory-tract bacteria, which were able to get into the lungs via the damaged bronchial tubes of the victims.[85] The virus also killed people directly by causing massive hemorrhages and edema in the lungs.[86]Modern analysis has shown the virus to be particularly deadly because it triggers a cytokine storm (overreaction of the body's immune system).[5] One group of researchers recovered the virus from the bodies of frozen victims and transfected animals with it. The animals suffered rapidly progressive respiratory failure and death through a cytokine storm. The strong immune reactions of young adults were postulated to have ravaged the body, whereas the weaker immune reactions of children and middle-aged adults resulted in fewer deaths among those groups.[78][87]
Misdiagnosis
Because the virus that caused the disease was too small to be seen under a microscope at the time, there were problems with correctly diagnosing it.[88] The bacterium haemophilus influenzae was instead mistakenly thought to be the cause, as it was big enough to be seen and was present in many, though not all, patients.[88] During the deadly second wave there were also fears that it was in fact plague, dengue fever, or cholera.[89] Another common misdiagnosis was typhus, which was common in circumstances of social upheaval, and was therefore also affecting Russia in the aftermath of the October Revolution.[89] In Chile, the view of the country's elite was that the nation was in severe decline, and therefore the assumption of doctors was that the disease was typhus caused by poor hygiene, and not an infectious one, causing a mismanaged response which did not ban mass gatherings.[89]
Responses

Public health management
While systems for alerting public health authorities of infectious spread did exist in 1918, they did not generally include influenza, leading to a delayed response.[90] Nevertheless, actions were taken. Maritime quarantines were declared on islands such as Iceland, Australia, and American Samoa, saving many lives.[90] Social distancing measures were introduced, for example closing schools, theatres, and places of worship, limiting public transportation, and banning mass gatherings.[91] Wearing face masks became common in some places, such as Japan, though there were debates over their efficacy.[91] There was also some resistance to their use, as exemplified by the Anti-Mask League of San Francisco. Vaccines were also developed, but as these were based on bacteria and not the actual virus, they could only help with secondary infections.[91] The actual enforcement of various restrictions varied.[92]
A later study found that measures such as banning mass gatherings and requiring the wearing of face masks could cut the death rate up to 50 percent, but this was dependent on them being imposed early in the outbreak and not being lifted prematurely.[93]
Medical treatment
As there were no antiviral drugs to treat the virus, and no antibiotics to treat the secondary bacterial infections, doctors would rely on a random assortment of medicines with varying degrees of effectiveness, such as aspirin, quinine, arsenics, digitalis, strychnine, epsom salts, castor oil, and iodine.[94] Treatments of traditional medicine, such as bloodletting, ayurveda, and kampo were also applied.[95]
Information dissemination
Due to World War I, many countries engaged in wartime censorship, and suppressed reporting of the pandemic.[96] For example, the Italian newspaper Corriere della Sera was prohibited from reporting daily death tolls.[97] The newspapers of the time were also generally paternalistic and worried about mass panic.[97] Misinformation would also spread along the disease. In Ireland there was a belief that noxious gases were rising from the mass graves of Flanders Fields and being "blown all over the world by winds".[98] There were also beliefs that the Germans were behind it, for example by poisoning the aspirin manufactured by Bayer, or by releasing poison gas from U-boats.[99]
Mortality
Around the globe


The Spanish flu infected around 500 million people, about one-third of the world's population.[2] Estimates as to how many infected people died vary greatly, but the flu is regardless considered to be one of the deadliest pandemics in history.[102][103] An estimate from 1991 states that the virus killed between 25 and 39 million people.[81] A 2005 estimate put the death toll at 50 million (about 3% of the global population), and possibly as high as 100 million (more than 5%).[80][104] However, a reassessment in 2018 estimated the total to be about 17 million,[105] though this has been contested.[106] With a world population of 1.8 to 1.9 billion,[107] these estimates correspond to between 1 and 6 percent of the population.
The disease killed in many parts of the world. Some 12-17 million people died in India, about 5% of the population.[108] The death toll in India's British-ruled districts was 13.88 million.[109] Another estimate gives at least 12 million dead.[110] The decade between 1911 and 1921 was the only census period in which India’s population fell, mostly due to devastation of the Spanish flu pandemic.[111][112]
In Finland, 20,000 died out of 210,000 infected.[113] In Sweden, 34,000 did.[114]
In Japan, 23 million people were affected, with at least 390,000 reported deaths.[115] In the Dutch East Indies (now Indonesia), 1.5 million were assumed to have died among 30 million inhabitants.[116] In Tahiti, 13% of the population died during one month. Similarly, in Western Samoa 22% of the population of 38,000 died within two months.[117]
In New Zealand, the flu killed an estimated 6,400 Pakeha and 2,500 indigenous Maori in six weeks, with Māori dying at eight times the rate of Pakeha.[118][119]
In the U.S., about 28% of the population of 105 million became infected, and 500,000 to 850,000 died (0.48 to 0.81 percent of the population).[120][121][122] Native American tribes were particularly hard hit. In the Four Corners area, there were 3,293 registered deaths among Native Americans.[123] Entire Inuit and Alaskan Native village communities died in Alaska.[124] In Canada, 50,000 died.[125]
In Brazil, 300,000 died, including president Rodrigues Alves.[126]
In Britain, as many as 250,000 died; in France, more than 400,000.[127]
In Ghana, the influenza epidemic killed at least 100,000 people.[128] Tafari Makonnen (the future Haile Selassie, Emperor of Ethiopia) was one of the first Ethiopians who contracted influenza but survived.[129][130] Many of his subjects did not; estimates for fatalities in the capital city, Addis Ababa, range from 5,000 to 10,000, or higher.[131]
The death toll in Russia has been estimated at 450,000, though the epidemiologists who suggested this number called it a "shot in the dark".[81] If it is correct, Russia lost roughly 0.4% of its population, meaning it suffered the lowest influenza-related mortality in Europe. Another study considers this number unlikely, given that the country was in the grip of a civil war, and the infrastructure of daily life had broken down; the study suggests that Russia's death toll was closer to 2%, or 2.7 million people.[132]
Devastated communities
Even in areas where mortality was low, so many adults were incapacitated that much of everyday life was hampered. Some communities closed all stores or required customers to leave orders outside. There were reports that healthcare workers could not tend the sick nor the gravediggers bury the dead because they too were ill. Mass graves were dug by steam shovel and bodies buried without coffins in many places.[133]
Bristol Bay, a region of Alaska populated by indigenous people, suffered a death rate of 40 percent of the total population, with some villages entirely disappearing.[134]
Several Pacific island territories were hit particularly hard. The pandemic reached them from New Zealand, which was too slow to implement measures to prevent ships, such as the SS Talune, carrying the flu from leaving its ports. From New Zealand, the flu reached Tonga (killing 8% of the population), Nauru (16%), and Fiji (5%, 9,000 people).[135] Worst affected was Western Samoa, formerly German Samoa, which had been occupied by New Zealand in 1914. 90% of the population was infected; 30% of adult men, 22% of adult women, and 10% of children died. By contrast, Governor John Martin Poyer prevented the flu from reaching neighboring American Samoa by imposing a blockade.[135] The disease spread fastest through the higher social classes among the indigenous peoples, because of the custom of gathering oral tradition from chiefs on their deathbeds; many community elders were infected through this process.[136]
In Iran, the mortality was very high: according to an estimate, between 902,400 and 2,431,000, or 8% to 22% of the total population died.[137] The country was going through the Persian famine of 1917–1919 concurrently.
In Ireland, during the worst 12 months, the Spanish flu accounted for one-third of all deaths.[138][139]
In South Africa it is estimated that about 300,000 people amounting to 6% of the population died within six weeks. Government actions in the early stages of the virus' arrival in the country in September 1918 are believed to have unintentionally accelerated its spread throughout the country.[140] Almost a quarter of the working population of Kimberley, consisting of workers in the diamond mines, died.[141] In British Somaliland, one official estimated that 7% of the native population died.[142] This huge death toll resulted from an extremely high infection rate of up to 50% and the extreme severity of the symptoms, suspected to be caused by cytokine storms.[81]
Less-affected areas
In the Pacific, American Samoa and the French colony of New Caledonia[144] also succeeded in preventing even a single death from influenza through effective quarantines. Australia also managed to avoid the first two waves with a quarantine.[90] Iceland protected a third of its population from exposure by blocking the main road of the island.[90] By the end of the pandemic, the isolated island of Marajó, in Brazil's Amazon River Delta had not reported an outbreak.[145] Saint Helena also reported no deaths.[146]

Estimates for the death toll in China have varied widely,[147][81] a range which reflects the lack of centralized collection of health data at the time due to the Warlord period. China may have experienced a relatively mild flu season in 1918 compared to other areas of the world.[65][66][69][148] However, some reports from its interior suggest that mortality rates from influenza were perhaps higher in at least a few locations in China in 1918.[132] At the very least, there is little evidence that China as a whole was seriously affected by the flu compared to other countries in the world.[149]
The first estimate of the Chinese death toll was made in 1991 by Patterson and Pyle, which estimated China had a death toll of between 5 and 9 million. However, this 1991 study was subsequently criticized by later studies due to flawed methodology, and newer studies have published estimates of a far lower mortality rate in China.[64][150][65] For instance, Iijima in 1998 estimates the death toll in China to be between 1 and 1.28 million based on data available from Chinese port cities.[151] The lower estimates of the Chinese death toll are based on the low mortality rates that were found in Chinese port cities (for example, Hong Kong) and on the assumption that poor communications prevented the flu from penetrating the interior of China.[147] However, some contemporary newspaper and post office reports, as well as reports from missionary doctors, suggest that the flu did penetrate the Chinese interior and that influenza was severe in at least some locations in the countryside of China.[132] Although medical records from China's interior are lacking, there was extensive medical data recorded in Chinese port cities, such as then British-controlled Hong Kong, Canton, Peking, Harbin and Shanghai. This data was collected by the Chinese Maritime Customs Service, which was largely staffed by non-Chinese foreigners, such as the British, French, and other European colonial officials in China.[152] As a whole, accurate data from China's port cities show astonishingly low mortality rates compared to other cities in Asia.[152] For example, the British authorities at Hong Kong and Canton reported a mortality rate from influenza at a rate of 0.25% and 0.32%, much lower than the reported mortality rate of other cities in Asia, such as Calcutta or Bombay, where influenza was much more devastating.[152][65] Similarly, in the city of Shanghai – which had a population of over 2 million in 1918 – there were only 266 recorded deaths from influenza among the Chinese population in 1918.[152] If extrapolated from the extensive data recorded from Chinese cities, the suggested mortality rate from influenza in China as a whole in 1918 was likely lower than 1% – much lower than the world average (which was around 3–5%).[152] In contrast, Japan and Taiwan had reported a mortality rate from influenza around 0.45% and 0.69% respectively, higher than the mortality rate collected from data in Chinese port cities, such as Hong Kong (0.25%), Canton (0.32%), and Shanghai.[152]
Patterns of fatality
.jpg)
The pandemic mostly killed young adults. In 1918–1919, 99% of pandemic influenza deaths in the U.S. occurred in people under 65, and nearly half of deaths were in young adults 20 to 40 years old. In 1920, the mortality rate among people under 65 had decreased sixfold to half the mortality rate of people over 65, but 92% of deaths still occurred in people under 65.[153] This is unusual, since influenza is typically most deadly to weak individuals, such as infants under age two, adults over age 70, and the immunocompromised. In 1918, older adults may have had partial protection caused by exposure to the 1889–1890 flu pandemic, known as the "Russian flu".[154] According to historian John M. Barry, the most vulnerable of all – "those most likely, of the most likely", to die – were pregnant women. He reported that in thirteen studies of hospitalized women in the pandemic, the death rate ranged from 23% to 71%.[155] Of the pregnant women who survived childbirth, over one-quarter (26%) lost the child.[156]Another oddity was that the outbreak was widespread in the summer and autumn (in the Northern Hemisphere); influenza is usually worse in winter.[157]
There were also geographic patterns to the disease's fatality. Some parts of Asia had 30 times higher death rates than some parts of Europe, and generally Africa and Asia had higher rates, while Europe, North America, and Asia had lower ones.[158] There was also great variation within continents, with three times higher mortality in Hungary and Spain compared to Denmark, two to three times higher chance of death in Sub-Saharan Africa compared to North Africa, and possibly up to ten times higher rates between the extremes of Asia.[158] Cities were affected worse than rural areas.[158] There were also differences between cities, which might have reflected exposure to the milder first wave giving immunity, as well as the introduction of social distancing measures.[159]
Another major pattern was that of differences between social classes. In Oslo, death rates were inversely correlated with apartment size, as the poorer people living in smaller apartments died at a higher rate.[160] Social status was also reflected in the higher mortality among immigrant communities, with Italian Americans, a recently arrived group at the time, were nearly twice as likely to die compared to the average Americans.[158] These disparities reflected worse diets, crowded living conditions, and problems accessing healthcare.[158] Paradoxically however, African Americans were relatively spared by the pandemic.[158]
More men than women were killed by the flu, as they were more likely to go out and be exposed, while women would tend to stay at home.[159] For the same reason men also were more likely to have pre-existing tuberculosis, which severely worsened the chances of recovery.[159] However, in India the opposite was true, potentially because Indian women were neglected with poorer nutrition, and were expected to care for the sick.[159]
A study conducted by He et al. (2011) used a mechanistic modeling approach to study the three waves of the 1918 influenza pandemic. They examined the factors that underlie variability in temporal patterns and their correlation to patterns of mortality and morbidity. Their analysis suggests that temporal variations in transmission rate provide the best explanation, and the variation in transmission required to generate these three waves is within biologically plausible values.[161] Another study by He et al. (2013) used a simple epidemic model incorporating three factors to infer the cause of the three waves of the 1918 influenza pandemic. These factors were school opening and closing, temperature changes throughout the outbreak, and human behavioral changes in response to the outbreak. Their modeling results showed that all three factors are important, but human behavioral responses showed the most significant effects.[162]
Impact
World War I
Academic Andrew Price-Smith has made the argument that the virus helped tip the balance of power in the latter days of the war towards the Allied cause. He provides data that the viral waves hit the Central Powers before the Allied powers and that both morbidity and mortality in Germany and Austria were considerably higher than in Britain and France.[59]
Economic

Many businesses in the entertainment and service industries suffered losses in revenue, while the healthcare industry reported profit gains.[163] Historian Nancy Bristow has argued that the pandemic, when combined with the increasing number of women attending college, contributed to the success of women in the field of nursing. This was due in part to the failure of medical doctors, who were predominantly men, to contain and prevent the illness. Nursing staff, who were mainly women, celebrated the success of their patient care and did not associate the spread of the disease with their work.[164]
A 2020 study found that US cities that implemented early and extensive non-medical measures (quarantine etc.) suffered no additional adverse economic effects due to implementing those measures,[165] when compared with cities that implemented measures late or not at all.[166]
Long-term effects
A 2006 study in the Journal of Political Economy found that "cohorts in utero during the pandemic displayed reduced educational attainment, increased rates of physical disability, lower income, lower socioeconomic status, and higher transfer payments received compared with other birth cohorts."[167] A 2018 study found that the pandemic reduced educational attainment in populations.[168] The flu has also been linked to the outbreak of encephalitis lethargica in the 1920s.[169]
Legacy
Despite the high morbidity and mortality rates that resulted from the epidemic, the Spanish flu began to fade from public awareness over the decades until the arrival of news about bird flu and other pandemics in the 1990s and 2000s.[170] This has led some historians to label the Spanish flu a "forgotten pandemic".[52]

There are various theories of why the Spanish flu was "forgotten". The rapid pace of the pandemic, which, for example, killed most of its victims in the United States within less than nine months, resulted in limited media coverage. The general population was familiar with patterns of pandemic disease in the late 19th and early 20th centuries: typhoid, yellow fever, diphtheria and cholera all occurred near the same time. These outbreaks probably lessened the significance of the influenza pandemic for the public.[171] In some areas, the flu was not reported on, the only mention being that of advertisements for medicines claiming to cure it.[172]
Additionally, the outbreak coincided with the deaths and media focus on the First World War.[173] Another explanation involves the age group affected by the disease. The majority of fatalities, from both the war and the epidemic, were among young adults. The number of war-related deaths of young adults may have overshadowed the deaths caused by flu.[153]
When people read the obituaries, they saw the war or postwar deaths and the deaths from the influenza side by side. Particularly in Europe, where the war's toll was high, the flu may not have had a tremendous psychological impact or may have seemed an extension of the war's tragedies.[153] The duration of the pandemic and the war could have also played a role. The disease would usually only affect a particular area for a month before leaving. The war, however, had initially been expected to end quickly but lasted for four years by the time the pandemic struck.
In 2019, the first dedicated monument to the memory of the pandemic was unveiled in Wiesloch in Germany.[174]
In fiction
- 1918, a 1985 American drama film.
- The Last Town on Earth, a 2006 novel.
- Spanish Flu: The Forgotten Fallen, a 2009 British television series.
- Awakenings, a 1990 American drama film.
Comparison with other pandemics
This flu killed more people in 24 weeks than HIV/AIDS killed in 24 years.[78] However, it killed a much lower percentage of the world's population than the Black Death, which lasted for many more years.[175]
| Name | Date | World pop. | Subtype | Reproduction number[178] | Infected (est.) | Deaths worldwide | Case fatality rate | Pandemic severity |
|---|---|---|---|---|---|---|---|---|
| 1889–90 flu pandemic[179] | 1889–90 | 1.53 billion | Likely H3N8 or H2N2 | 2.10 (IQR, 1.9–2.4)[179] | 20–60%[179] (300–900 million) | 1 million | 0.10–0.28%[179] | 2 |
| 1918 flu[180] | 1918–20 | 1.80 billion | H1N1 | 1.80 (IQR, 1.47–2.27) | 33% (500 million)[181] or >56% (>1 billion)[182] | 17[183] – 100[184][185] million | 2–3%,[182] or ~4%, or ~10%[186] | 5 |
| Asian flu | 1957–58 | 2.90 billion | H2N2 | 1.65 (IQR, 1.53–1.70) | >17% (>500 million)[182] | 1–4 million[182] | <0.2%[182] | 2 |
| Hong Kong flu | 1968–69 | 3.53 billion | H3N2 | 1.80 (IQR, 1.56–1.85) | >14% (>500 million)[182] | 1–4 million[182] | <0.2%[182] | 2 |
| 2009 flu pandemic[187][188] | 2009–10 | 6.85 billion | H1N1/09 | 1.46 (IQR, 1.30–1.70) | 11-21% (0.7–1.4 billion)[189] | 151,700 – 575,400[190] | 0.03%[191] | 1 |
| Typical seasonal flu[t 1] | Every year | 7.75 billion | A/H3N2, A/H1N1, B, ... | 1.28 (IQR, 1.19–1.37) | 5–15% (340 million – 1 billion)[192] 3–11% or 5–20%[193][194] (240 million–1.6 billion) |
290,000 – 650,000/year[195] | <0.1%[196] | 1 |
Notes
| ||||||||
Research
The origin of the Spanish flu pandemic, and the relationship between the near-simultaneous outbreaks in humans and swine, have been controversial. One hypothesis is that the virus strain originated at Fort Riley, Kansas, in viruses in poultry and swine which the fort bred for food; the soldiers were then sent from Fort Riley around the world, where they spread the disease.[197] Similarities between a reconstruction of the virus and avian viruses, combined with the human pandemic preceding the first reports of influenza in swine, led researchers to conclude the influenza virus jumped directly from birds to humans, and swine caught the disease from humans.[198][199] Others have disagreed,[200] and more recent research has suggested the strain may have originated in a nonhuman, mammalian species.[201] An estimated date for its appearance in mammalian hosts has been put at the period 1882–1913.[202] This ancestor virus diverged about 1913–1915 into two clades (or biological groups), which gave rise to the classical swine and human H1N1 influenza lineages. The last common ancestor of human strains dates to between February 1917 and April 1918. Because pigs are more readily infected with avian influenza viruses than are humans, they were suggested as the original recipients of the virus, passing the virus to humans sometime between 1913 and 1918.

An effort to recreate the 1918 flu strain (a subtype of avian strain H1N1) was a collaboration among the Armed Forces Institute of Pathology, the USDA ARS Southeast Poultry Research Laboratory, and Mount Sinai School of Medicine in New York City. The effort resulted in the announcement (on 5 October 2005) that the group had successfully determined the virus's genetic sequence, using historic tissue samples recovered by pathologist Johan Hultin from an Inuit female flu victim buried in the Alaskan permafrost and samples preserved from American soldiers[203] Roscoe Vaughan and James Downs.[204][205]
On 18 January 2007, Kobasa et al. (2007) reported that monkeys (Macaca fascicularis) infected with the recreated flu strain exhibited classic symptoms of the 1918 pandemic, and died from cytokine storms[206] – an overreaction of the immune system. This may explain why the 1918 flu had its surprising effect on younger, healthier people, as a person with a stronger immune system would potentially have a stronger overreaction.[207]
On 16 September 2008, the body of British politician and diplomat Sir Mark Sykes was exhumed to study the RNA of the flu virus in efforts to understand the genetic structure of modern H5N1 bird flu. Sykes had been buried in 1919 in a lead coffin which scientists hoped had helped preserve the virus.[208] The coffin was found to be split and the cadaver badly decomposed; nonetheless, samples of lung and brain tissue were taken.[209]
In December 2008, research by Yoshihiro Kawaoka of the University of Wisconsin linked the presence of three specific genes (termed PA, PB1, and PB2) and a nucleoprotein derived from 1918 flu samples to the ability of the flu virus to invade the lungs and cause pneumonia. The combination triggered similar symptoms in animal testing.[210]
In June 2010, a team at the Mount Sinai School of Medicine reported the 2009 flu pandemic vaccine provided some cross-protection against the 1918 flu pandemic strain.[211]
One of the few things known for certain about the influenza in 1918 and for some years after was that it was, except in the laboratory, exclusively a disease of human beings.[212]
In 2013, the AIR Worldwide Research and Modeling Group "characterized the historic 1918 pandemic and estimated the effects of a similar pandemic occurring today using the AIR Pandemic Flu Model". In the model, "a modern day 'Spanish flu' event would result in additional life insurance losses of between US$15.3–27.8 billion in the United States alone", with 188,000–337,000 deaths in the United States.[213]
In 2018, Michael Worobey, an evolutionary biology professor at the University of Arizona who is examining the history of the 1918 pandemic, revealed that he obtained tissue slides created by William Rolland, a physician who reported on a respiratory illness likely to be the virus while a pathologist in the British military during World War One.[214] Rolland had authored an article in the Lancet during 1917 about a respiratory illness outbreak beginning in 1916 in Étaples, France.[215][216] Worobey traced recent references to that article to family members who had retained slides that Rolland had prepared during that time. Worobey extracted tissue from the slides to potentially reveal more about the origin of the pathogen.
See also
References
Citations
- Yang, Wan; Petkova, Elisaveta; Shaman, Jeffrey (2014). "The 1918 influenza pandemic in New York City: age-specific timing, mortality, and transmission dynamics". Influenza and Other Respiratory Viruses. 8 (2): 177–188. doi:10.1111/irv.12217. PMC 4082668. PMID 24299150.
- Taubenberger & Morens 2006.
- Rosenwald MS (7 April 2020). "History's deadliest pandemics, from ancient Rome to modern America". Washington Post. Archived from the original on 7 April 2020. Retrieved 11 April 2020.
- Gagnon A, Miller MS, Hallman SA, Bourbeau R, Herring DA, Earn DJ, Madrenas J (2013). "Age-specific mortality during the 1918 influenza pandemic: unravelling the mystery of high young adult mortality". PLOS ONE. 8 (8): e69586. Bibcode:2013PLoSO...869586G. doi:10.1371/journal.pone.0069586. PMC 3734171. PMID 23940526.
- Barry 2004b.
- MacCallum WG (1919). "Pathology of the pneumonia following influenza". JAMA: The Journal of the American Medical Association. 72 (10): 720–23. doi:10.1001/jama.1919.02610100028012. Archived from the original on 25 January 2020. Retrieved 16 August 2019.
- Hirsch EF, McKinney M (1919). "An epidemic of pneumococcus broncho-pneumonia". Journal of Infectious Diseases. 24 (6): 594–617. doi:10.1093/infdis/24.6.594. JSTOR 30080493.
- Brundage JF, Shanks GD (December 2007). "What really happened during the 1918 influenza pandemic? The importance of bacterial secondary infections". The Journal of Infectious Diseases. 196 (11): 1717–18, author reply 1718–19. doi:10.1086/522355. PMID 18008258.
- Morens DM, Fauci AS (April 2007). "The 1918 influenza pandemic: insights for the 21st century". The Journal of Infectious Diseases. 195 (7): 1018–28. doi:10.1086/511989. PMID 17330793.
- "La Grippe Espagnole de 1918" (in French). Institut Pasteur. Archived from the original (Powerpoint) on 17 November 2015. (also here, requires Flash player)
- Porras-Gallo & Davis 2014.
- Galvin 2007.
- "Spanish flu facts". Channel 4 News. Archived from the original on 27 January 2010.
- Anderson S (29 August 2006). "Analysis of Spanish flu cases in 1918–1920 suggests transfusions might help in bird flu pandemic". American College of Physicians. Archived from the original on 25 November 2011. Retrieved 2 October 2011.
- Barry 2004, p. 171.
- Spinney 2018, p. 58.
- Davis 2013, pp. 103–36.
- Harvey J (18 March 2020). "Yes, Viruses Used To Be Named After Places. Here's Why They Aren't Anymore". Retrieved 8 April 2020.
- "WHO issues best practices for naming new human infectious diseases". World Health Organization. 8 May 2015. Retrieved 8 April 2020.
- "Pandemic influenza: an evolving challenge". World Health Organization. 22 May 2018. Archived from the original on 20 March 2020. Retrieved 20 March 2020.
- "Influenza pandemic of 1918–19". Encyclopaedia Britannica. 4 March 2020. Archived from the original on 20 March 2020. Retrieved 20 March 2020.
- Chodosh S (18 March 2020). "What the 1918 flu pandemic can teach us about COVID-19, in four charts". PopSci. Retrieved 20 March 2020.
- Spinney, Laura (2018). Pale rider: the Spanish flu of 1918 and how it changed the world. Vintage. p. 36. ISBN 978-1-78470-240-3. OCLC 1090305029.
- Barry, John M (20 January 2004). "The site of origin of the 1918 influenza pandemic and its public health implications". Journal of Translational Medicine. 2. doi:10.1186/1479-5876-2-3. ISSN 1479-5876. PMID 14733617.
- "1918 Flu (Spanish flu epidemic)". Avian Bird Flu. Archived from the original on 21 May 2008.
- "Spanish flu strikes during World War I". 14 January 2010. Archived from the original on 11 December 2013.
- Billings 1997.
- "The Memoirs of Herbert Hoover: Years of Adventure, 1874–1920. (New York: Macmillan Company. 1951. Pp. xi, 496. $4.00.) and Herbert Hoover and the Russian Prisoners of World War I: A Study in Diplomacy and Relief, 1918–1919. By Edward F. Willis. (Stanford: Stanford University Press. 1951. Pp. viii, 67. $1.50.)". The American Historical Review: 12. 2011. doi:10.1086/ahr/57.3.709. ISSN 1937-5239.
- Spinney, Laura (2018). Pale rider: the Spanish flu of 1918 and how it changed the world. Vintage. p. 37. ISBN 978-1-78470-240-3. OCLC 1090305029.
- "Queer Epidemic Sweeps North China; Banks and Silk Stores in Peking Closed—Another Loan Sought from Japan". The New York Times. June 1, 1918. ISSN 0362-4331. Retrieved June 22, 2020.
- Patterson, K. David; Pyle, Gerald F. (1991). "The Geography and Mortality of the 1918 Influenza Pandemic". Bulletin of the History of Medicine. 65 (1): 4–21. JSTOR 44447656. PMID 2021692.
- Taubenberger, Jeffery K.; Morens, David M. (2006). "1918 Influenza: the Mother of All Pandemics". Emerging Infectious Diseases. 12 (1): 15–22. doi:10.3201/eid1201.050979. PMC 3291398. PMID 16494711.
- "Mortality Statistics 1918: Nineteenth Annual Report" (PDF). United States Census Bureau. 1920. p. 28. Retrieved 29 May 2020.
- Erkoreka, Anton (2010). "The Spanish influenza pandemic in occidental Europe (1918–1920) and victim age". Influenza and Other Respiratory Viruses. 4 (2): 81–89. doi:10.1111/j.1750-2659.2009.00125.x. PMC 5779284. PMID 20167048.
- Spinney, Laura. (2018). Pale rider : the Spanish flu of 1918 and how it changed the world. Vintage. p. 38. ISBN 978-1-78470-240-3. OCLC 1090305029.
- Byerly CR (April 2010). "The U.S. military and the influenza pandemic of 1918-1919". Public Health Reports. 125 Suppl 3: 82–91. PMC 2862337. PMID 20568570.
- Spinney, Laura. (2018). Pale rider : the Spanish flu of 1918 and how it changed the world. Vintage. p. 39. ISBN 978-1-78470-240-3. OCLC 1090305029.
- Spinney, Laura. (2018). Pale rider : the Spanish flu of 1918 and how it changed the world. Vintage. p. 40. ISBN 978-1-78470-240-3. OCLC 1090305029.
- Spinney, Laura. (2018). Pale rider : the Spanish flu of 1918 and how it changed the world. Vintage. p. 41. ISBN 978-1-78470-240-3. OCLC 1090305029.
- Spinney, Laura. (2018). Pale rider : the Spanish flu of 1918 and how it changed the world. Vintage. p. 42. ISBN 978-1-78470-240-3. OCLC 1090305029.
- Kenner, Robert (18 January 2010). "Influenza 1918". American Experience. Season 10. Episode 5. PBS. WGBH. Transcript.
- Why the Second Wave of the 1918 Spanish Flu Was So Deadly History.com - Retrieved 8 May 2020
- Radusin M (2012). "The Spanish Flu – Part II: the second and third wave". Vojnosanitetski Pregled. 69 (10): 917–27. PMID 23155616. Retrieved 23 April 2020.
- "1918 Pandemic Influenza: Three Waves". Centers for Disease Control and Prevention. 11 May 2018. Retrieved 23 April 2020.
- Najera RF (2 January 2019). "Influenza in 1919 and 100 Years Later". College of Physicians of Philadelphia. Retrieved 23 April 2020.
- "Here are Exact Facts About the Influenza and Its Toll in City, State, Nation, world". Los Angeles Times. 9 February 1919. Retrieved 10 May 2020.
- Yang W, Petkova E, Shaman J (March 2014). "The 1918 influenza pandemic in New York City: age-specific timing, mortality, and transmission dynamics". Influenza and Other Respiratory Viruses. National Institutes of Health. 8 (2): 177–88. doi:10.1111/irv.12217. PMC 4082668. PMID 24299150.
- Warren T. Vaughan (July 1921). "Influenza: An Epidemiologic Study". American Journal of Hygiene. Retrieved 11 May 2020.
- "Mortality Statistics 1919: Twentieth Annual Report" (PDF). United States Census Bureau. 1921. p. 30. Retrieved 11 May 2020.
- "How the 1918 flu pandemic rolled on for years: a snapshot from 1920". The Guardian. Retrieved 30 April 2020.
- Spinney, Laura. (2018). Pale rider : the Spanish flu of 1918 and how it changed the world. Vintage. p. 43. ISBN 978-1-78470-240-3. OCLC 1090305029.
- Crosby 2003.
- Worobey, Michael; Cox, Jim; Gill, Douglas (2019). "The origins of the great pandemic". Evolution, Medicine, and Public Health. 2019 (1): 18–25.
- Vikki Valentine (20 February 2006). "Origins of the 1918 Pandemic: The Case for France". National Public Radio. Archived from the original on 20 April 2009. Retrieved 13 April 2020.
- Oxford JS (December 2001). "The so-called Great Spanish Influenza Pandemic of 1918 may have originated in France in 1916". Philosophical Transactions of the Royal Society of London. Series B, Biological Sciences. Royal Society. 356 (1416): 1857–59. doi:10.1098/rstb.2001.1012. PMC 1088561. PMID 11779384.
- Connor S (8 January 2000). "Flu epidemic traced to Great War transit camp". The Guardian. UK. Archived from the original on 12 May 2009. Retrieved 9 May 2009.
- Oxford JS, Lambkin R, Sefton A, Daniels R, Elliot A, Brown R, Gill D (January 2005). "A hypothesis: the , gas, pigs, ducks, geese and horses in northern France during the Great War provided the conditions for the emergence of the "Spanish" influenza pandemic of 1918-1919" (PDF). Vaccine. 23 (7): 940–45. doi:10.1016/j.vaccine.2004.06.035. PMID 15603896. Archived (PDF) from the original on 12 March 2020. Retrieved 12 March 2020.
- Shanks GD (January 2016). "No evidence of 1918 influenza pandemic origin in Chinese laborers/soldiers in France". Journal of the Chinese Medical Association. 79 (1): 46–48. doi:10.1016/j.jcma.2015.08.009. PMID 26542935.
- Price-Smith 2008.
- Hannoun C (1993). "La Grippe". Documents de la Conférence de l'Institut Pasteur. La Grippe Espagnole de 1918. Ed Techniques Encyclopédie Médico-Chirurgicale (EMC), Maladies infectieuses. 8-069-A-10.
- Humphries 2014.
- Vergano D (24 January 2014). "1918 Flu Pandemic That Killed 50 Million Originated in China, Historians Say". National Geographic. Archived from the original on 26 January 2014. Retrieved 4 November 2016.
- Spinney, Laura. (2018). Pale rider : the Spanish flu of 1918 and how it changed the world. Vintage. p. 143. ISBN 978-1-78470-240-3. OCLC 1090305029.
- Killingray D, Phillips H (2003). The Spanish Influenza Pandemic of 1918–1919: New Perspectives. Routledge. ISBN 978-1-134-56640-2.
- Langford C (2005). "Did the 1918-19 Influenza Pandemic Originate in China?". Population and Development Review. 31 (3): 473–505. doi:10.1111/j.1728-4457.2005.00080.x. JSTOR 3401475.
- Cheng KF, Leung PC (July 2007). "What happened in China during the 1918 influenza pandemic?". International Journal of Infectious Diseases. 11 (4): 360–64. doi:10.1016/j.ijid.2006.07.009. PMID 17379558.
- Klein C. "China Epicenter of 1918 Flu Pandemic, Historian Says". History.com. Archived from the original on 5 March 2020. Retrieved 5 March 2020.
- Vergano D. "1918 Flu Pandemic That Killed 50 Million Originated in China, Historians Say". National Geographic. Archived from the original on 3 March 2020. Retrieved 5 March 2020.
- Saunders-Hastings PR, Krewski D (December 2016). "Reviewing the History of Pandemic Influenza: Understanding Patterns of Emergence and Transmission". Pathogens. 5 (4): 66. doi:10.3390/pathogens5040066. PMC 5198166. PMID 27929449.
- Mills, Christina E.; Robins, James M.; Lipsitch, Marc (16 December 2004). "Transmissibility of 1918 pandemic influenza". Nature. 432 (7019): 904–906. doi:10.1038/nature03063. ISSN 1476-4687. PMC 7095078. PMID 15602562.
- Qureshi 2016, p. 42.
- Ewald 1994.
- Illing S (20 March 2020). "The most important lesson of the 1918 influenza pandemic: Tell the damn truth". Vox. Archived from the original on 25 March 2020.
John M. Barry : The government lied. They lied about everything. We were at war and they lied because they didn’t want to upend the war effort. You had public health leaders telling people this was just the ordinary flu by another name. They simply didn’t tell the people the truth about what was happening.
- Gladwell 1997, p. 55.
- Gladwell 1997, p. 63.
- Fogarty International Center. "Summer Flu Outbreak of 1918 May Have Provided Partial Protection Against Lethal Fall Pandemic". Fic.nih.gov. Archived from the original on 27 July 2011. Retrieved 19 May 2012.
- Gladwell 1997, p. 56.
- Barry 2004.
- Spinney, Laura. (2018). Pale rider : the Spanish flu of 1918 and how it changed the world. Vintage. pp. 45–47. ISBN 978-1-78470-240-3. OCLC 1090305029.
- Knobler 2005.
- Patterson & Pyle 1991.
- Morris DE, Cleary DW, Clarke SC (2017). "Secondary Bacterial Infections Associated with Influenza Pandemics". Frontiers in Microbiology. 8: 1041. doi:10.3389/fmicb.2017.01041. PMC 5481322. PMID 28690590.
- "Bacterial Pneumonia Caused Most Deaths in 1918 Influenza Pandemic". National Institutes of Health. 23 September 2015. Archived from the original on 22 April 2016. Retrieved 17 April 2016.
- Taubenberger et al. 2001, pp. 1829–1839.
- Morens, David M.; Taubenberger, Jeffery K.; Fauci, Anthony S. (1 October 2008). "Predominant Role of Bacterial Pneumonia as a Cause of Death in Pandemic Influenza: Implications for Pandemic Influenza Preparedness". The Journal of infectious diseases. 198 (7): 962–970. doi:10.1086/591708. ISSN 0022-1899. PMC 2599911. PMID 18710327.
- Taubenberger et al. 2001, pp. 1829–39.
- "1918 Death Certificate for 10-year-old girl who died as a consequence of influenza in Lares, Puerto Rico".
- Spinney, Laura. (2018). Pale rider : the Spanish flu of 1918 and how it changed the world. Vintage. p. 61. ISBN 978-1-78470-240-3. OCLC 1090305029.
- Spinney, Laura. (2018). Pale rider : the Spanish flu of 1918 and how it changed the world. Vintage. p. 62. ISBN 978-1-78470-240-3. OCLC 1090305029.
- Spinney, Laura. (2018). Pale rider : the Spanish flu of 1918 and how it changed the world. Vintage. pp. 83–4. ISBN 978-1-78470-240-3. OCLC 1090305029.
- Spinney, Laura. (2018). Pale rider : the Spanish flu of 1918 and how it changed the world. Vintage. pp. 87–8. ISBN 978-1-78470-240-3. OCLC 1090305029.
- Spinney, Laura. (2018). Pale rider : the Spanish flu of 1918 and how it changed the world. Vintage. p. 91. ISBN 978-1-78470-240-3. OCLC 1090305029.
- Bootsma, Martin C. J.; Ferguson, Neil M. (6 April 2007). "The effect of public health measures on the 1918 influenza pandemic in U.S. cities". Proceedings of the National Academy of Sciences. 104 (18): 7588–7593. doi:10.1073/pnas.0611071104. ISSN 0027-8424.
- Spinney, Laura. (2018). Pale rider : the Spanish flu of 1918 and how it changed the world. Vintage. pp. 109–110. ISBN 978-1-78470-240-3. OCLC 1090305029.
- Spinney, Laura. (2018). Pale rider : the Spanish flu of 1918 and how it changed the world. Vintage. pp. 111–112. ISBN 978-1-78470-240-3. OCLC 1090305029.
- Little, Becky. "As the 1918 Flu Emerged, Cover-Up and Denial Helped It Spread". HISTORY. Retrieved 23 June 2020.
- Spinney, Laura. (2018). Pale rider : the Spanish flu of 1918 and how it changed the world. Vintage. p. 92. ISBN 978-1-78470-240-3. OCLC 1090305029.
- Spinney, Laura. (2018). Pale rider : the Spanish flu of 1918 and how it changed the world. Vintage. p. 69. ISBN 978-1-78470-240-3. OCLC 1090305029.
- Spinney, Laura. (2018). Pale rider : the Spanish flu of 1918 and how it changed the world. Vintage. p. 70. ISBN 978-1-78470-240-3. OCLC 1090305029.
- Taubenberger & Morens 2006, p. 19.
- Taubenberger & Morens 2006, p. 17.
- "Ten things you need to know about pandemic influenza (update of 14 October 2005)" (PDF). Releve Epidemiologique Hebdomadaire. 80 (49–50): 428–31. December 2005. PMID 16372665.
- Jilani TN, Jamil RT, Siddiqui AH (14 December 2019). "H1N1 Influenza (Swine Flu)". StatPearls. Treasure Island (FL): StatPearls. PMID 30020613. Archived from the original on 12 March 2020. Retrieved 11 March 2020 – via NCBI.
- Johnson & Mueller 2002.
- Spreeuwenberg P, Kroneman M, Paget J (December 2018). "Reassessing the Global Mortality Burden of the 1918 Influenza Pandemic". Am. J. Epidemiol. 187 (12): 2561–2567. doi:10.1093/aje/kwy191. PMC 7314216. PMID 30202996.
- Chandra S, Christensen J (July 2019). "Re: "reassessing the Global Mortality Burden of the 1918 Influenza Pandemic"". American Journal of Epidemiology. 188 (7): 1404–06. doi:10.1093/aje/kwz044. PMID 30824934. and response Spreeuwenberg P, Kroneman M, Paget J (July 2019). "The Authors Reply" (PDF). American Journal of Epidemiology. 188 (7): 1405–06. doi:10.1093/aje/kwz041. PMID 30824908. Archived (PDF) from the original on 12 March 2020. Retrieved 12 March 2020.
- "Historical Estimates of World Population". Archived from the original on 9 July 2012. Retrieved 29 March 2013.
- Mayor S (October 2000). "Flu experts warn of need for pandemic plans". BMJ. 321 (7265): 852. doi:10.1136/bmj.321.7265.852. PMC 1118673. PMID 11021855.
- Chandra, Kuljanin & Wray 2012.
- David Arnold, "Dearth and the Modern Empire: The 1918–19 Influenza Epidemic in India," Transactions of the Royal Historical Society 29 (2019): 181–200.
- "Why 1918 matters in India's corona war".
- "What the history of pandemics tells us about coronavirus".
- "Historiallisia Papereita 1 - ISSN 1456-8055". historiallinenyhdistys.fi. Retrieved 24 June 2020.
- Åman, Margareta (1990). Spanska sjukan: den svenska epidemin 1918-1920 och dess internationella bakgrund (in Swedish). Uppsala; Stockholm: Ubsaliensis Academiae ; Distributor, Almqvist & Wiksell International. ISBN 978-91-554-2587-6. OCLC 22451542.
- "Spanish Influenza in Japanese Armed Forces, 1918–1920". Centers for Disease Control and Prevention (CDC).
- Historical research report from University of Indonesia, School of History, as reported in Emmy Fitri. Looking Through Indonesia's History For Answers to Swine Flu Archived 2 November 2009 at the Wayback Machine. The Jakarta Globe. 28 October 2009 edition.
- Kohn 2007.
- "1918 flu centenary: How to survive a pandemic". Archived from the original on 9 July 2019. Retrieved 19 June 2019.
- Rice G, Bryder L. Black November: the 1918 influenza pandemic in New Zealand (Second, revised and enlarged ed.). Christchurch, N.Z. ISBN 978-1927145913. OCLC 960210402.
- "1918-1920 — Influenza and Pneumonia Pandemic — Nationwide ~820,000-850,000 – Deadliest American Disasters and Large-Loss-of-Life Events".
- The Great Pandemic: The United States in 1918–1919, U.S. Department of Health & Human Services.
- "The silent invader - Digital Collections - National Library of Medicine".
- "Flu Epidemic Hit Utah Hard in 1918, 1919". 28 March 1995. Archived from the original on 30 November 2012. Retrieved 7 July 2012.
- "The Great Pandemic of 1918: State by State". 5 March 2018. Archived from the original on 6 May 2009. Retrieved 4 May 2009.
- "A deadly virus rages throughout Canada at the end of the First World War". CBC History.
- "A gripe espanhola no Brasil – Elísio Augusto de Medeiros e Silva, empresário, escritor e membro da AEILIJ" (in Portuguese). Jornal de Hoje. Archived from the original on 2 February 2014. Retrieved 22 January 2014.
- "The "bird flu" that killed 40 million". BBC News. 19 October 2005. Archived from the original on 7 November 2017. Retrieved 26 April 2009.
- Hays 1998.
- Marcus H (1996). Haile Sellassie I: The formative years, 1892–1936. Trenton, NJ: Red Sea Press. pp. 36ff.
- Pankhurst 1991, pp. 48f.
- Pankhurst 1991, p. 63.
- Spinney L (2017). Pale rider – The Spanish flu of 1918 and how it changed the world. pp. 167–69. ISBN 978-1-910702-37-6.
- "Viruses of mass destruction". cnn.com. Fortune. 1 November 2004. Archived from the original on 6 May 2009. Retrieved 30 April 2009.
- Spinney, Laura. (2018). Pale rider : the Spanish flu of 1918 and how it changed the world. Vintage. p. 134. ISBN 978-1-78470-240-3. OCLC 1090305029.
- Denoon 2004.
- Wishart S (July–August 2018). "How the 1918 flu spread". New Zealand Geographic (152): 23. Archived from the original on 3 August 2018. Retrieved 3 August 2018.
- Afkhami 2003; Afkhami 2012.
- FitzGerald, John. "Coronavirus: forgotten lessons of the Spanish flu pandemic". The Irish Times. Retrieved 14 June 2020.
Yet the “Spanish” flu epidemic of 1918-19 resulted in about 25,000 extra deaths in Ireland, many of them young adults. This was almost as many deaths as occurred among the Irish fighting in the First World War.
- "Official Ireland Statistics Office". Central Statistics Office Ireland. Retrieved 14 June 2020.
Total deaths in Ireland 1916: 50,627
- Phillips, Howard. "South Africa bungled the Spanish flu in 1918. History mustn't repeat itself for COVID-19". The Conversation. Retrieved 26 May 2020.
- Spinney, Laura. (2018). Pale rider : the Spanish flu of 1918 and how it changed the world. Vintage. p. 72. ISBN 978-1-78470-240-3. OCLC 1090305029.
- Pankhurst 1991, pp. 51ff.
- Bell D, Nicoll A, Fukuda K, Horby P, Monto A, Hayden F, et al. (January 2006). "Non-pharmaceutical interventions for pandemic influenza, international measures". Emerging Infectious Diseases. 12 (1): 81–87. doi:10.3201/eid1201.051370. PMC 3291414. PMID 16494722.
- Ryan, Jeffrey, ed. (2009). Pandemic Influenza: Emergency planning and community preparedness. Boca Raton, FL: CRC Press. p. 24.
- "Colonial Annual Report", 1919
- Iijima W (2003). "Spanish influenza in China, 1918–1920: a preliminary probe". In Phillips H, Killingray D (eds.). The Spanish Flu Pandemic of 1918: New Perspectives. London and New York: Routledge. pp. 101–09.
- Killingray D, Phillips H (2003). The Spanish Influenza Pandemic of 1918–1919: New Perspectives. Routledge. ISBN 978-1-134-56640-2.
- Killingray D, Phillips H (2003). The Spanish Influenza Pandemic of 1918-1919: New Perspectives. Routledge. ISBN 978-1-134-56640-2.
- Iijima W (1998). The Spanish influenza in China, 1918–1920. OCLC 46987588.
- Iijima W (1998). The Spanish influenza in China, 1918–1920. Spanish 'Flu 1918-1998: Reflections on the Influenza Pandemic of 1918 after 80 Years. Cape Town, South Africa.
- Killingray D, Phillips H (2003). The Spanish Influenza Pandemic of 1918–1919: New Perspectives. Routledge. ISBN 978-1-134-56640-2.
- Simonsen et al. 1998.
- Hanssen, Olav. Undersøkelser over influenzaens optræden specielt i Bergen 1918–1922. Bg. 1923. 66 s. ill. (Haukeland sykehus. Med. avd. Arb. 2) (Klaus Hanssens fond. Skr. 3)
- Payne MS, Bayatibojakhi S (2014). "Exploring preterm birth as a polymicrobial disease: an overview of the uterine microbiome". Frontiers in Immunology. 5: 595. doi:10.3389/fimmu.2014.00595. PMC 4245917. PMID 25505898.
- Barry 2004, p. 239.
- "Key Facts about Swine Influenza". Archived from the original on 4 May 2009. Retrieved 30 April 2009.
- Spinney, Laura. (2018). Pale rider : the Spanish flu of 1918 and how it changed the world. Vintage. pp. 180–182. ISBN 978-1-78470-240-3. OCLC 1090305029.
- Spinney, Laura. (2018). Pale rider : the Spanish flu of 1918 and how it changed the world. Vintage. pp. 183–184. ISBN 978-1-78470-240-3. OCLC 1090305029.
- Mamelund, Svenn-Erik (February 2006). "A socially neutral disease? Individual social class, household wealth and mortality from Spanish influenza in two socially contrasting parishes in Kristiania 1918–19". Social Science & Medicine. 62 (4): 923–940. doi:10.1016/j.socscimed.2005.06.051. ISSN 0277-9536.
- He et al. 2011.
- He et al. 2013.
- Garret 2007.
- Lindley R. "The Forgotten American Pandemic: Historian Dr. Nancy K. Bristow on the Influenza Epidemic of 1918". hnn.us. Archived from the original on 8 August 2014. Retrieved 4 August 2014.
- "What can the Spanish Flu teach us about the COVID-19 pandemic?". World Economic Forum. 2 April 2020.
- Correia S, Luck S, Verner E (2020). "Pandemics Depress the Economy, Public Health Interventions Do Not: Evidence from the 1918 Flu". SSRN Working Paper Series. doi:10.2139/ssrn.3561560. ISSN 1556-5068.
- Almond, Douglas (1 August 2006). "Is the 1918 Influenza Pandemic Over? Long‐Term Effects of In Utero Influenza Exposure in the Post‐1940 U.S. Population". Journal of Political Economy. 114 (4): 672–712. doi:10.1086/507154. ISSN 0022-3808.
- Beach B, Ferrie JP, Saavedra MH (2018). "Fetal shock or selection? The 1918 influenza pandemic and human capital development". nber.org. doi:10.3386/w24725. Archived from the original on 18 June 2018. Retrieved 18 June 2018.
- Vilensky, Foley & Gilman 2007.
- Honigsbaum 2008.
- Morrisey 1986.
- Benedict & Braithwaite 2000, p. 38.
- Crosby 2003, pp. 320–22.
- "Wiesloch: Ein alter Grabstein will zum Nachdenken anregen". www.rnz.de (in German). Retrieved 27 June 2020.
- Meyer R (29 April 2016). "Human extinction isn't that unlikely". The Atlantic. Archived from the original on 1 May 2016. Retrieved 6 February 2018.
- Hilleman MR (August 2002). "Realities and enigmas of human viral influenza: pathogenesis, epidemiology and control". Vaccine. 20 (25–26): 3068–87. doi:10.1016/S0264-410X(02)00254-2. PMID 12163258.
- Potter CW (October 2001). "A history of influenza". Journal of Applied Microbiology. 91 (4): 572–9. doi:10.1046/j.1365-2672.2001.01492.x. PMID 11576290.
- Biggerstaff M, Cauchemez S, Reed C, Gambhir M, Finelli L (September 2014). "Estimates of the reproduction number for seasonal, pandemic, and zoonotic influenza: a systematic review of the literature". BMC Infectious Diseases. 14 (1): 480. doi:10.1186/1471-2334-14-480. PMC 4169819. PMID 25186370.
- Valleron AJ, Cori A, Valtat S, Meurisse S, Carrat F, Boëlle PY (May 2010). "Transmissibility and geographic spread of the 1889 influenza pandemic". Proceedings of the National Academy of Sciences of the United States of America. 107 (19): 8778–81. Bibcode:2010PNAS..107.8778V. doi:10.1073/pnas.1000886107. PMC 2889325. PMID 20421481.
- Mills CE, Robins JM, Lipsitch M (December 2004). "Transmissibility of 1918 pandemic influenza". Nature. 432 (7019): 904–6. Bibcode:2004Natur.432..904M. doi:10.1038/nature03063. PMC 7095078. PMID 15602562.
- Taubenberger JK, Morens DM (January 2006). "1918 Influenza: the mother of all pandemics". Emerging Infectious Diseases. 12 (1): 15–22. doi:10.3201/eid1201.050979. PMC 3291398. PMID 16494711.
- "Report of the Review Committee on the Functioning of the International Health Regulations (2005) in relation to Pandemic (H1N1) 2009" (PDF). 5 May 2011. p. 37. Archived (PDF) from the original on 14 May 2015. Retrieved 1 March 2015.
- Spreeuwenberg P, Kroneman M, Paget J (December 2018). "Reassessing the Global Mortality Burden of the 1918 Influenza Pandemic". American Journal of Epidemiology. 187 (12): 2561–2567. doi:10.1093/aje/kwy191. PMID 30202996.
- Morens DM, Fauci AS (April 2007). "The 1918 influenza pandemic: insights for the 21st century". The Journal of Infectious Diseases. 195 (7): 1018–28. doi:10.1086/511989. PMID 17330793.
- Johnson NP, Mueller J (2002). "Updating the accounts: global mortality of the 1918-1920 "Spanish" influenza pandemic". Bulletin of the History of Medicine. 76 (1): 105–15. doi:10.1353/bhm.2002.0022. PMID 11875246.
- Lin II R, Karlamangla S (6 March 2020). "Why the coronavirus outbreak isn't likely to be a repeat of the 1918 Spanish flu". Los Angeles Times.
- Donaldson LJ, Rutter PD, Ellis BM, Greaves FE, Mytton OT, Pebody RG, Yardley IE (December 2009). "Mortality from pandemic A/H1N1 2009 influenza in England: public health surveillance study". BMJ. 339: b5213. doi:10.1136/bmj.b5213. PMC 2791802. PMID 20007665.
- "First Global Estimates of 2009 H1N1 Pandemic Mortality Released by CDC-Led Collaboration". Centers for Disease Control and Prevention (CDC). 25 June 2012. Retrieved 7 July 2012.
- Kelly H, Peck HA, Laurie KL, Wu P, Nishiura H, Cowling BJ (5 August 2011). "The age-specific cumulative incidence of infection with pandemic influenza H1N1 2009 was similar in various countries prior to vaccination". PLOS One. 6 (8): e21828. Bibcode:2011PLoSO...621828K. doi:10.1371/journal.pone.0021828. PMC 3151238. PMID 21850217.
- Dawood FS, Iuliano AD, Reed C, Meltzer MI, Shay DK, Cheng PY, et al. (September 2012). "Estimated global mortality associated with the first 12 months of 2009 pandemic influenza A H1N1 virus circulation: a modelling study". The Lancet. Infectious Diseases. 12 (9): 687–95. doi:10.1016/S1473-3099(12)70121-4. PMID 22738893.
- Triggle N (10 December 2009). "Swine flu less lethal than feared". BBC News. BBC News Online. Archived from the original on 13 December 2009. Retrieved 10 December 2009.
- "WHO Europe – Influenza". World Health Organization (WHO). June 2009. Archived from the original on 17 June 2009. Retrieved 12 June 2009.
- CDC (28 October 2019). "Key Facts About Influenza (Flu)". cdc.gov. citing Tokars, Olsen& Reed (2018). Retrieved 10 March 2020.
- Tokars JI, Olsen SJ, Reed C (May 2018). "Seasonal Incidence of Symptomatic Influenza in the United States". Clinical Infectious Diseases. 66 (10): 1511–1518. doi:10.1093/cid/cix1060. PMC 5934309. PMID 29206909.
- "Influenza: Fact sheet". World Health Organization (WHO). 6 November 2018. Archived from the original on 17 December 2019. Retrieved 25 January 2020.
- "H1N1 fatality rates comparable to seasonal flu". The Malaysian Insider. Washington, D.C., USA. Reuters. 17 September 2009. Archived from the original on 20 October 2009. Retrieved 26 September 2009.
- "Open Collections Program: Contagion, Spanish Influenza in North America, 1918–1919". Archived from the original on 20 November 2016. Retrieved 22 November 2016.
- Harder TC, Ortrud W. "Chapter Two: Avian Influenza". Influenza Report 2006. published online.
Sometimes a virus contains both avian-adapted genes and human-adapted genes. Both the H2N2 and H3N2 pandemic strains contained avian flu virus RNA segments. "While the pandemic human influenza viruses of 1957 (H2N2) and 1968 (H3N2) clearly arose through reassortment between human and avian viruses, the influenza virus causing the 'Spanish flu' in 1918 appears to be entirely derived from an avian source (Belshe 2005).
- Taubenberger et al. 2005.
- Antonovics, Hood & Baker 2006.
- Vana & Westover 2008.
- dos Reis, Hay & Goldstein 2009.
- "Researchers reconstruct 1918 pandemic influenza virus; effort designed to advance preparedness". Center for Disease Control. Archived from the original on 19 October 2011. Retrieved 2 September 2009.
- "Closing In On a Killer: Scientists Unlock Clues to the Spanish Influenz Virus". National Museum of Health and Medicine. Retrieved 23 March 2020.
- Kolata G (16 February 1999). "Scientists Uncover Clues To Flu Epidemic of 1918". The New York Times. Retrieved 23 March 2020.
- Kobasa & et al. 2007.
- "Research on monkeys finds resurrected 1918 flu killed by turning the body against itself". USA Today. Archived from the original on 5 March 2009. Retrieved 14 August 2008.
- "Body exhumed in fight against flu". BBC News. Archived from the original on 17 September 2008. Retrieved 16 September 2008.
- In Search of Spanish Flu (documentary). BBC Four.
- Fox 2008.
- Fox 2010.
- Crosby 1976, p. 295.
- Madhav 2013.
- Branswell H (5 December 2018). "A shot-in-the-dark e-mail leads to a century-old family treasure – and hope of cracking a deadly flu's secret". Stat. Archived from the original on 5 December 2018. Retrieved 5 December 2018.
- Hammond J, Rolland W, Shore T (14 July 1917). "Purulent bronchitis: A study of cases occurring amongst the British troops at a base in France". The Lancet. 190 (4898): 41–45. doi:10.1016/S0140-6736(01)56229-7. PDF version here Archived 26 August 2019 at the Wayback Machine
- "The Influenza Pandemic of 1918". World War 1 Centenary. Oxford, England: University of Oxford. Archived from the original on 9 December 2018. Retrieved 8 December 2018.
Bibliography
- Antonovics J, Hood ME, Baker CH (April 2006). "Molecular virology: was the 1918 flu avian in origin?". Nature. 440 (7088): E9, discussion E9–10. Bibcode:2006Natur.440E...9A. doi:10.1038/nature04824. PMID 16641950.CS1 maint: ref=harv (link)
- Afkhami A (2003). "Compromised constitutions: the Iranian experience with the 1918 influenza pandemic". Bulletin of the History of Medicine. 77 (2): 367–92. doi:10.1353/bhm.2003.0049. PMID 12955964. – Open access material by the Psychiatry and Behavioral Sciences at Health Sciences Research Commons.
- Afkhami A (29 March 2012) [15 December 2004]. "Influenza". In Yarshater E (ed.). Encyclopædia Iranica. Fasc. 2. XIII (Online ed.). New York City: Bibliotheca Persica Press. pp. 140–143.
- Barry JM (2004). The Great Influenza: The Epic Story of the Greatest Plague in History. Viking Penguin. ISBN 978-0-670-89473-4.CS1 maint: ref=harv (link)
- Barry, John M. (January 2004). "The site of origin of the 1918 influenza pandemic and its public health implications". Journal of Translational Medicine. 2 (1): 3. doi:10.1186/1479-5876-2-3. PMC 340389. PMID 14733617.
- Benedict ML, Braithwaite M (2000). "The Year of the Killer Flu". In the Face of Disaster: True Stories of Canadian Heroes from the Archives of Maclean's. New York: Viking. p. 38. ISBN 978-0-670-88883-2.CS1 maint: ref=harv (link)
- Billings M (1997). "The 1918 Influenza Pandemic". Virology at Stanford University. Archived from the original on 4 May 2009. Retrieved 1 May 2009.CS1 maint: ref=harv (link)
- Bristow, Nancy K. American Pandemic: The Lost Worlds of the 1918 Influenza Epidemic (OUP, 2012)
- "1918 Influenza: the Mother of All Pandemics". Archived from the original on 1 October 2009. Retrieved 2 September 2009.CS1 maint: ref=harv (link)
- Chandra S, Kuljanin G, Wray J (August 2012). "Mortality from the influenza pandemic of 1918–1919: the case of India". Demography. 49 (3): 857–65. doi:10.1007/s13524-012-0116-x. PMID 22661303.CS1 maint: ref=harv (link)
- Crosby AW (1976). Epidemic and Peace, 1918. Westport, CT: Greenwood Press. ISBN 978-0-8371-8376-3.CS1 maint: ref=harv (link)
- Crosby AW (2003). America's Forgotten Pandemic: The Influenza of 1918 (2nd ed.). Cambridge University Press. ISBN 978-0-521-54175-6 – via Google Books.CS1 maint: ref=harv (link)
- Davis RA (2013). The Spanish Flu: Narrative and Cultural Identity in Spain, 1918. Palgrave Macmillan. ISBN 978-1-137-33921-8 – via Google Books.CS1 maint: ref=harv (link)
- Denoon D (2004). "New Economic Orders: Land, Labour and Dependency". In Denoon D (ed.). The Cambridge History of the Pacific Islanders. CUP. p. 247. ISBN 978-0-521-00354-4.CS1 maint: ref=harv (link)
- dos Reis M, Hay AJ, Goldstein RA (October 2009). "Using non-homogeneous models of nucleotide substitution to identify host shift events: application to the origin of the 1918 'Spanish' influenza pandemic virus". Journal of Molecular Evolution. Springer Science and Business Media LLC. 69 (4): 333–45. Bibcode:2009JMolE..69..333D. doi:10.1007/s00239-009-9282-x. PMC 2772961. PMID 19787384.CS1 maint: ref=harv (link)
- Ewald PW (1994). Evolution of infectious disease. OUP. ISBN 978-0-19-506058-4.CS1 maint: ref=harv (link)
- Fox M (29 December 2008). "Researchers unlock secrets of 1918 flu pandemic". Reuters. Retrieved 2 September 2009.CS1 maint: ref=harv (link)
- Fox M (16 June 2010). "Swine flu shot protects against 1918 flu: study". Reuters.CS1 maint: ref=harv (link)
- Galvin J (31 July 2007). "Spanish Flu Pandemic: 1918". Popular Mechanics. Retrieved 2 October 2011.CS1 maint: ref=harv (link)
- Garret TA (2007). Economic Effects of the 1918 Influenza Pandemic: Implications for a Modern-day Pandemic (PDF).CS1 maint: ref=harv (link)
- Gladwell M (29 September 1997). "The Dead Zone". The New Yorker.CS1 maint: ref=harv (link)
- Hays JN (1998). The Burdens of Disease: Epidemics and Human Response in Western History. p. 274. ISBN 978-0-8135-2528-0 – via Google Books.CS1 maint: ref=harv (link)
- He DH, Dushoff J, Day T, Ma J, Earn DJ (2011). "Mechanistic modelling of the three waves of the 1918 influenza pandemic". Theoretical Ecology. 4 (2): 283–88. doi:10.1007/s12080-011-0123-3. ISSN 1874-1738.CS1 maint: ref=harv (link)
- He D, Dushoff J, Day T, Ma J, Earn DJ (September 2013). "Inferring the causes of the three waves of the 1918 influenza pandemic in England and Wales". Proceedings. Biological Sciences. 280 (1766): 20131345. doi:10.1098/rspb.2013.1345. PMC 3730600. PMID 23843396.CS1 maint: ref=harv (link)
- Honigsbaum M (2008). Living with Enza: The Forgotten Story of Britain and the Great Flu Pandemic of 1918. Palgrave Macmillan. ISBN 978-0-230-21774-4.CS1 maint: ref=harv (link)
- Humphries MO (2014). "Paths of Infection: The First World War and the Origins of the 1918 Influenza Pandemic". War in History. 21 (1): 55–81. doi:10.1177/0968344513504525.CS1 maint: ref=harv (link)
- Johnson NP, Mueller J (2002). "Updating the accounts: global mortality of the 1918-1920 "Spanish" influenza pandemic". Bulletin of the History of Medicine. 76 (1): 105–15. doi:10.1353/bhm.2002.0022. PMID 11875246.CS1 maint: ref=harv (link)
- Knobler S, Mack A, Mahmoud A, Lemon S, eds. (2005). "1: The Story of Influenza". The Threat of Pandemic Influenza: Are We Ready? Workshop Summary (2005). Washington, DC: The National Academies Press. pp. 60–61.
- Kobasa D, Jones SM, Shinya K, Kash JC, Copps J, Ebihara H, et al. (January 2007). "Aberrant innate immune response in lethal infection of macaques with the 1918 influenza virus". Nature. 445 (7125): 319–23. Bibcode:2007Natur.445..319K. doi:10.1038/nature05495. PMID 17230189.
- Kohn GC (2007). Encyclopedia of plague and pestilence: from ancient times to the present (3rd ed.). Infobase Publishing. p. 363. ISBN 978-0-8160-6935-4 – via Google Books.CS1 maint: ref=harv (link)
- Madhav, Nita (February 2013). "Modeling a Modern Day Spanish Flu Pandemic" (PDF). AIR Worldwide. Retrieved 5 May 2020.CS1 maint: ref=harv (link)
- Morrisey CR (1986). "The Influenza Epidemic of 1918". Navy Medicine. 77 (3): 11–17.CS1 maint: ref=harv (link)
- Noymer A, Carreon D, Johnson N (April 2010). "Questioning the salicylates and influenza pandemic mortality hypothesis in 1918-1919". Clinical Infectious Diseases. 50 (8): 1203, author reply 1203. doi:10.1086/651472. PMID 20233050.CS1 maint: ref=harv (link)
- Pankhurst R (1991). An Introduction to the Medical History of Ethiopia. Trenton: Red Sea Press. ISBN 978-0-932415-45-5.CS1 maint: ref=harv (link)
- Patterson KD, Pyle GF (1991). "The geography and mortality of the 1918 influenza pandemic". Bulletin of the History of Medicine. 65 (1): 4–21. PMID 2021692.CS1 maint: ref=harv (link)
- Porras-Gallo M, Davis RA, eds. (2014). "The Spanish Influenza Pandemic of 1918–1919: Perspectives from the Iberian Peninsula and the Americas". Rochester Studies in Medical History. 30. University of Rochester Press. ISBN 978-1-58046-496-3 – via Google Books.CS1 maint: ref=harv (link)
- Price-Smith AT (2008). Contagion and Chaos. Cambridge, MA: MIT Press. ISBN 978-0-262-66203-1.CS1 maint: ref=harv (link)
- Qureshi AI (2016). Ebola Virus Disease: From Origin to Outbreak. Academic Press. ISBN 978-0128042427 – via Google Books.CS1 maint: ref=harv (link)
- Rice GW (2005). Black November; the 1918 Influenza Pandemic in New Zealand (2nd ed.). University of Canterbury Press. ISBN 978-1-877257-35-3.CS1 maint: ref=harv (link)
- Simonsen L, Clarke MJ, Schonberger LB, Arden NH, Cox NJ, Fukuda K (July 1998). "Pandemic versus epidemic influenza mortality: a pattern of changing age distribution". The Journal of Infectious Diseases. 178 (1): 53–60. CiteSeerX 10.1.1.327.2581. doi:10.1086/515616. JSTOR 30114117. PMID 9652423.CS1 maint: ref=harv (link)
- Spinney, Laura (2018). Pale rider: the Spanish flu of 1918 and how it changed the world. London: Vintage. ISBN 978-1-78470-240-3. OCLC 1090305029.
- Starko KM (November 2009). "Salicylates and pandemic influenza mortality, 1918-1919 pharmacology, pathology, and historic evidence". Clinical Infectious Diseases. 49 (9): 1405–10. doi:10.1086/606060. PMID 19788357.CS1 maint: ref=harv (link) (summary by Infectious Diseases Society of America and ScienceDaily, 3 October 2009)
- Starko KM (2010). "Reply to Noymer et al" (PDF). Clinical Infectious Diseases. 50 (8): 1203–04. doi:10.1086/651473.CS1 maint: ref=harv (link)
- Taubenberger JK, Reid AH, Janczewski TA, Fanning TG (December 2001). "Integrating historical, clinical and molecular genetic data in order to explain the origin and virulence of the 1918 Spanish influenza virus". Philosophical Transactions of the Royal Society of London. Series B, Biological Sciences. 356 (1416): 1829–39. doi:10.1098/rstb.2001.1020. PMC 1088558. PMID 11779381.CS1 maint: ref=harv (link)
- Taubenberger JK, Reid AH, Lourens RM, Wang R, Jin G, Fanning TG (October 2005). "Characterization of the 1918 influenza virus polymerase genes". Nature. 437 (7060): 889–93. Bibcode:2005Natur.437..889T. doi:10.1038/nature04230. PMID 16208372.CS1 maint: ref=harv (link)
- Taubenberger JK, Morens DM (January 2006). "1918 Influenza: the mother of all pandemics". Emerging Infectious Diseases. 12 (1): 15–22. doi:10.3201/eid1201.050979. PMC 3291398. PMID 16494711.CS1 maint: ref=harv (link)
- Vana G, Westover KM (June 2008). "Origin of the 1918 Spanish influenza virus: a comparative genomic analysis". Molecular Phylogenetics and Evolution. 47 (3): 1100–10. doi:10.1016/j.ympev.2008.02.003. PMID 18353690.CS1 maint: ref=harv (link)
- Vilensky JA, Foley P, Gilman S (August 2007). "Children and encephalitis lethargica: a historical review". Pediatric Neurology. 37 (2): 79–84. doi:10.1016/j.pediatrneurol.2007.04.012. PMID 17675021.CS1 maint: ref=harv (link)
Further reading
- Beiner, Guy (1 October 2006). "Out in the Cold and Back: New-Found Interest in the Great Flu". Cultural and Social History. 3 (4): 496–505. doi:10.1191/1478003806cs070ra (inactive 29 May 2020).
- Brown J (2018). Influenza: The Hundred Year Hunt to Cure the Deadliest Disease in History. New York: Atria. ISBN 978-1501181245.
- Collier R (1974). The Plague of the Spanish Lady – The Influenza Pandemic of 1918–19. Atheneum. ISBN 978-0-689-10592-0.
- Dorratoltaj N (29 March 2018). Carrell H (ed.). "What the 1918 Flu Pandemic Can Teach Today's Insurers". AIR Research and Modeling Group. Retrieved 28 May 2019.
- Duncan K (2003). Hunting the 1918 flu: one scientist's search for a killer virus (illustrated ed.). University of Toronto Press. ISBN 978-0-8020-8748-5.
- Humphries, Mark Osborne (2013). The Last Plague: Spanish Influenza and the Politics of Public Health in Canada. University of Toronto Press. ISBN 978-1-4426-1044-6.
- Johnson N (2006). Britain and the 1918–19 Influenza Pandemic: A Dark Epilogue. London and New York: Routledge. ISBN 978-0-415-36560-4.
- Johnson N (2003). "Measuring a pandemic: Mortality, demography and geography". Popolazione e Storia: 31–52.
- Johnson N (2003). "Scottish 'flu – The Scottish mortality experience of the 'Spanish flu'". Scottish Historical Review. 83 (2): 216–26. doi:10.3366/shr.2004.83.2.216.
- Kolata G (1999). Flu: The Story of the Great Influenza Pandemic of 1918 and the Search for the Virus That Caused It. New York: Farrar, Straus and Giroux. ISBN 978-0-374-15706-7.
- Little J (2007). If I Die Before I Wake: The Flu Epidemic Diary of Fiona Macgregor, Toronto, Ontario, 1918. Dear Canada. Markham, Ont.: Scholastic Canada. ISBN 978-0-439-98837-7.
- Noymer A, Garenne M (2000). "The 1918 influenza epidemic's effects on sex differentials in mortality in the United States". Population and Development Review. 26 (3): 565–81. doi:10.1111/j.1728-4457.2000.00565.x. PMC 2740912. PMID 19530360.
- Oxford JS, Sefton A, Jackson R, Innes W, Daniels RS, Johnson NP (February 2002). "World War I may have allowed the emergence of 'Spanish' influenza". The Lancet. Infectious Diseases. 2 (2): 111–14. doi:10.1016/S1473-3099(02)00185-8. PMID 11901642.
- Oxford JS, Sefton A, Jackson R, Johnson NP, Daniels RS (December 1999). "Who's that lady?". Nature Medicine. 5 (12): 1351–52. doi:10.1038/70913. PMID 10581070.
- Pettit D, Bailie J (2008). A Cruel Wind: Pandemic Flu in America, 1918–1920. Murfreesboro, TN: Timberlane Books. ISBN 978-0-9715428-2-2.
- Philips H (2010). "The re-appearing shadow of 1918: trends in the historiography of the 1918–19 influenza pandemic". Canadian Bulletin of Medical History. 21 (1): 121–34. doi:10.3138/cbmh.21.1.121. PMID 15202430.
- Phillips, H. (1 September 2014). "The Recent Wave of 'Spanish' Flu Historiography". Social History of Medicine. 27 (4): 789–808. doi:10.1093/shm/hku066.
- Phillips H, Killingray D, eds. (2003). The Spanish Flu Pandemic of 1918: New Perspectives. London and New York: Routledge.
- Potter CW (October 2001). "A history of influenza". Journal of Applied Microbiology. 91 (4): 572–79. doi:10.1046/j.1365-2672.2001.01492.x. PMID 11576290.
- Rice GW, Palmer E (1993). "Pandemic Influenza in Japan, 1918–1919: Mortality Patterns and Official Responses". Journal of Japanese Studies. 19 (2): 389–420. doi:10.2307/132645. JSTOR 132645.
- Tumpey TM, García-Sastre A, Mikulasova A, Taubenberger JK, Swayne DE, Palese P, Basler CF (October 2002). "Existing antivirals are effective against influenza viruses with genes from the 1918 pandemic virus". Proceedings of the National Academy of Sciences of the United States of America. 99 (21): 13849–54. Bibcode:2002PNAS...9913849T. doi:10.1073/pnas.212519699. PMC 129786. PMID 12368467.
- Videos
- Presentation by Nancy Bristow on the Influenza Pandemic and World War I, November 1, 2019, C-SPAN
- "Spanish Flu: a warning from history". Cambridge University. 30 November 2018.
External links

| Wikiquote has quotations related to: Spanish flu |
- The American Influenza Epidemic of 1918–1919: A Digital Encyclopedia Largest digital collection of newspapers, archival manuscripts and interpretive essays exploring the impact of the epidemic on 50 U.S. cities (Univ. of Michigan).
- Spanish Flu: The History Channel WebSite (26 March 2020)
| Authority control |
|
|---|