Abdominal pain
| Abdominal pain | |
|---|---|
| Synonyms | Stomach ache, tummy ache, belly pain |
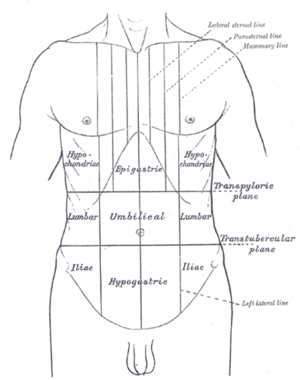 | |
| Abdominal pain can be characterized by the region it affects | |
| Classification and external resources | |
| Specialty | General surgery |
| Patient UK | Abdominal pain |
Abdominal pain, also known as a stomach ache, is a symptom associated with both non-serious and serious medical issues.
Common causes of pain in the abdomen include gastroenteritis and irritable bowel syndrome.[1] About 10% of people have a more serious underlying condition such as appendicitis, leaking or ruptured abdominal aortic aneurysm, diverticulitis, or ectopic pregnancy.[1] In a third of cases the exact cause is unclear.[1]
Given that a variety of diseases can cause some form of abdominal pain, a systematic approach to examination of a person and the formulation of a differential diagnosis remains important.
Diagnostic approach
In order to better understand the underlying cause of abdominal pain, one can perform a thorough history and physical examination.
The process of gathering a history may include:[2]
- Identifying more information about the chief complaint by eliciting a history of present illness; i.e. a narrative of the current symptoms such as the onset, location, duration, character, aggravating or relieving factors, and temporal nature of the pain. Identifying other possible factors may aid in the diagnosis of the underlying cause of abdominal pain, such as recent travel, recent contact with other ill individuals, and for females, a thorough gynecologic history.
- Learning about the patient's past medical history, focusing on any prior issues or surgical procedures.
- Clarifying the patient's current medication regimen, including prescriptions, over-the-counter medications, and supplements.
- Confirming the patient's drug and food allergies.
- Discussing with the patient any family history of disease processes, focusing on conditions that might resemble the patient's current presentation.
- Discussing with the patient any health-related behaviors (e.g. tobacco use, alcohol consumption, drug use, and sexual activity) that might make certain diagnoses more likely.
- Reviewing the presence of non-abdominal symptoms (e.g., fever, chills, chest pain, shortness of breath, vaginal bleeding) that can further clarify the diagnostic picture.
After gathering a thorough history, one should perform a physical exam in order to identify important physical signs that might clarify the diagnosis, including a cardiovascular exam, lung exam, thorough abdominal exam, and for females, a genitourinary exam.[2]
Additional investigations that can aid diagnosis include:[3]
- Blood tests including complete blood count, basic metabolic panel, electrolytes, liver function tests, amylase, lipase, troponin I, and for females, a serum pregnancy test.
- Urinalysis
- Imaging including chest and abdominal X-rays
- Electrocardiogram
If diagnosis remains unclear after history, examination, and basic investigations as above, then more advanced investigations may reveal a diagnosis. Such tests include:[3]
- Computed tomography of the abdomen/pelvis
- Abdominal or pelvic ultrasound
- Endoscopy and/or colonoscopy
Differential diagnosis
The most frequent reasons for abdominal pain are gastroenteritis (13%), irritable bowel syndrome (8%), urinary tract problems (5%), inflammation of the stomach (5%) and constipation (5%). In about 30% of cases, the cause is not determined. About 10% of cases have a more serious cause including gallbladder (gallstones or biliary dyskinesia) or pancreas problems (4%), diverticulitis (3%), appendicitis (2%) and cancer (1%).[1] More common in those who are older, mesenteric ischemia and abdominal aortic aneurysms are other serious causes.[4]
A more extensive list includes the following:
- Gastrointestinal
- GI tract
- Inflammatory: gastroenteritis, appendicitis, gastritis, esophagitis, diverticulitis, Crohn's disease, ulcerative colitis, microscopic colitis
- Obstruction: hernia, intussusception, volvulus, post-surgical adhesions, tumors, severe constipation, hemorrhoids
- Vascular: embolism, thrombosis, hemorrhage, sickle cell disease, abdominal angina, blood vessel compression (such as celiac artery compression syndrome), superior mesenteric artery syndrome, postural orthostatic tachycardia syndrome
- Digestive: peptic ulcer, lactose intolerance, celiac disease, food allergies
- Glands
- Bile system
- Inflammatory: cholecystitis, cholangitis
- Obstruction: cholelithiasis, tumours
- Liver
- Inflammatory: hepatitis, liver abscess
- Pancreatic
- Inflammatory: pancreatitis
- Bile system
- GI tract
- Renal and urological
- Inflammation: pyelonephritis, bladder infection, indigestion
- Obstruction: kidney stones, urolithiasis, urinary retention, tumours
- Vascular: left renal vein entrapment
- Gynaecological or obstetric
- Inflammatory: pelvic inflammatory disease
- Mechanical: ovarian torsion
- Endocrinological: menstruation, Mittelschmerz
- Tumors: endometriosis, fibroids, ovarian cyst, ovarian cancer
- Pregnancy: ruptured ectopic pregnancy, threatened abortion
- Abdominal wall
- muscle strain or trauma
- muscular infection
- neurogenic pain: herpes zoster, radiculitis in Lyme disease, abdominal cutaneous nerve entrapment syndrome (ACNES), tabes dorsalis
- Referred pain
- from the thorax: pneumonia, pulmonary embolism, ischemic heart disease, pericarditis
- from the spine: radiculitis
- from the genitals: testicular torsion
- Metabolic disturbance
- uremia, diabetic ketoacidosis, porphyria, C1-esterase inhibitor deficiency, adrenal insufficiency, lead poisoning, black widow spider bite, narcotic withdrawal
- Blood vessels
- Immune system
- Idiopathic
- irritable bowel syndrome (affecting up to 20% of the population, IBS is the most common cause of recurrent, intermittent abdominal pain)
Acute abdominal pain
Acute abdomen can be defined as severe, persistent abdominal pain of sudden onset that is likely to require surgical intervention to treat its cause. The pain may frequently be associated with nausea and vomiting, abdominal distention, fever and signs of shock. One of the most common conditions associated with acute abdominal pain is acute appendicitis.
Selected causes
- Traumatic: blunt or perforating trauma to the stomach, bowel, spleen, liver, or kidney
- Inflammatory:
- Infections such as appendicitis, cholecystitis, pancreatitis, pyelonephritis, pelvic inflammatory disease, hepatitis, mesenteric adenitis, or a subdiaphragmatic abscess
- Perforation of a peptic ulcer, a diverticulum, or the caecum
- Complications of inflammatory bowel disease such as Crohn's disease or ulcerative colitis
- Mechanical:
- Small bowel obstruction secondary to adhesions caused by previous surgeries, intussusception, hernias, benign or malignant neoplasms
- Large bowel obstruction caused by colorectal cancer, inflammatory bowel disease, volvulus, fecal impaction or hernia
- Vascular: occlusive intestinal ischemia, usually caused by thromboembolism of the superior mesenteric artery
By location
Location:[5]
- Upper middle abdominal pain
- Stomach (gastritis, stomach ulcer, stomach cancer)
- Pancreas pain (pancreatitis or pancreatic cancer, can radiate to the left side of the waist, back, and even shoulder)
- Duodenal ulcer, diverticulitis
- Appendicitis (starts here, after some time moves to lower right abdomen)
- Upper right abdominal pain
- Liver (caused by hepatomegaly due to fatty liver, hepatitis, or caused by liver cancer, abscess)
- Gallbladder and biliary tract (inflammation, gallstones, worm infection)
- Colon pain (below the area of liver – bowel obstruction, functional disorders, gas accumulation, spasm, inflammation, colon cancer)
- Upper left abdominal pain
- Spleen pain (splenomegaly)
- Pancreas
- Colon pain (below the area of spleen – bowel obstruction, functional disorders, gas accumulation, spasm, inflammation, colon cancer)
- Middle abdominal pain (pain in the area around belly button)
- Appendicitis (starts here)
- Small intestine pain (inflammation, intestinal spasm, functional disorders)
- Lower abdominal pain (diarrhea, colitis and dysentery)
- Lower right abdominal pain
- Cecum (intussusception, bowel obstruction)
- Appendix point (Appendicitis location)
- Lower left abdominal pain
- diverticulitis, sigmoid colon volvulus, obstruction or gas accumulation
- Pelvic pain
- bladder (cystitis, may be secondary to diverticulum and bladder stone, bladder cancer)
- pain in women (uterus, ovaries, fallopian tubes)
- Right low back pain
- liver pain (hepatomegaly)
- right kidney pain (its location below the area of liver pain)
- Left low back pain
- less in spleen pain
- left kidney pain
- Low back pain
- kidney pain (kidney stone, kidney cancer, hydronephrosis)
- Ureteral stone pain
Management
Butylscopolamine (Buscopan) is used to treat cramping abdominal pain with some success.[6]
Epidemiology
Abdominal pain is the reason about 3% of adults see their family physician.[1] Rates of emergency department visits in the United States for abdominal pain increased 18% from 2006 through 2011. This was the largest increase out of 20 common conditions seen in the ED. The rate of ED use for nausea and vomiting also increased 18%.[7]
References
- 1 2 3 4 5 Viniol, A; Keunecke, C; Biroga, T; Stadje, R; Dornieden, K; Bösner, S; Donner-Banzhoff, N; Haasenritter, J; Becker, A (October 2014). "Studies of the symptom abdominal pain--a systematic review and meta-analysis". Family practice. 31 (5): 517–29. doi:10.1093/fampra/cmu036. PMID 24987023.
- 1 2 Bickley, Lynn (2016). Bates' Guide to Physical Examination & History Taking. Philadelphia, Pennsylvania: Lippincott Williams & Wilkins. ISBN 9781469893419.
- 1 2 Cartwright, Sarah L.; Knudson, Mark P. (2008-04-01). "Evaluation of Acute Abdominal Pain in Adults". American Family Physician. 77 (7). ISSN 0002-838X.
- ↑ Spangler, R; Van Pham, T; Khoujah, D; Martinez, JP (2014). "Abdominal emergencies in the geriatric patient". International journal of emergency medicine. 7: 43. doi:10.1186/s12245-014-0043-2. PMC 4306086. PMID 25635203.
- ↑ Richard F.LeBlond. Diagnostics. US: McGraw-Hill Companies, Inc. ISBN 0-07-140923-8.
- ↑ Tytgat GN (2007). "Hyoscine butylbromide: a review of its use in the treatment of abdominal cramping and pain". Drugs. 67 (9): 1343–57. doi:10.2165/00003495-200767090-00007. PMID 17547475.
- ↑ Skiner HG, Blanchard J, Elixhauser A (September 2014). "Trends in Emergency Department Visits, 2006-2011". HCUP Statistical Brief #179. Rockville, MD: Agency for Healthcare Research and Quality.
External links
| Classification | |
|---|---|
| External resources |