HLA-B27
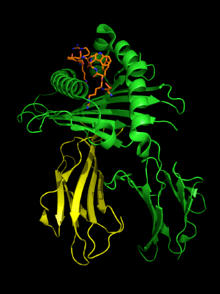 HLA-B*2705-peptide (chain A shown in green cartoon, chain B shown in yellow cartoon) complexed to a fragment of the influenza nucleoprotein NP383-391 (orange, sticks). PDB ID 2BST | ||
| B*2705-β2MG with bound peptide 2bst | ||
major histocompatibility complex (human), class I, B27 | ||
| Alleles | B*2701, 2702, 2703, . . . | |
| Structure (See HLA-B) | Available 3D structures | |
| EBI-HLA | B*2701 | |
| B*2702 | ||
| B*2703 | ||
| B*2704 | ||
| B*2705 | 2bsr, 2bss, 2bst, 2a83, 1w0v, 1uxs, 1ogt, 1hsa, 1jgd, 1jge | |
| B*2706 | ||
| B*2709 | 1w0w, 1uxw, 1of2, 1k5n | |
Human leukocyte antigen (HLA) B27 (subtypes B*2701-2759)[1] is a class I surface antigen encoded by the B locus in the major histocompatibility complex (MHC) on chromosome 6 and presents antigenic peptides (derived from self and non-self antigens) to T cells. HLA-B27 is strongly associated with ankylosing spondylitis (AS), and other associated inflammatory diseases referred to as "spondyloarthropathies". Diseases associated with the HLA-B27 subtype can be remembered with the mnemonic PAIR, and include Psoriasis, Ankylosing spondylitis, Inflammatory bowel disease, and Reactive arthritis.
The prevalence of HLA-B27 varies markedly in the general population. For example, about 8% of Caucasians, 4% of North Africans, 2-9% of Chinese, and 0.1-0.5% of persons of Japanese descent possess the gene that codes for this antigen.[1] In northern Scandinavia (Lapland), 24% of people are HLA-B27 positive, while 1.8% have associated ankylosing spondylitis.
A small group (<0.5%) of people infected with HIV are able to remain symptom-free for many years without medication. These long-term nonprogressors appear to be significantly common among people who are HLA-B27 positive.[2]
Disease associations
The relationship between HLA-B27 and many diseases has not yet been fully elucidated. Though it is associated with a wide range of pathology, particularly seronegative spondyloarthropathy, it does not appear to be the sole mediator in development of disease. For example, while 90% of people with ankylosing spondylitis (AS) are HLA-B27 positive, only a small fraction of people with HLA-B27 ever develop AS. People who are HLA-B27 positive are more likely to experience early onset AS than HLA-B27 negative individuals.[3] There are additional genes being discovered that also predispose to AS and associated diseases.[4] Additionally there are potential environmental factors (triggers) that may also play a role in susceptible individuals.[1]
Pathological mechanism
Due to its strong association with spondyloarthropathies, HLA-B27 is the most studied HLA-B allele. It is not entirely clear how HLA-B27 influences disease, however there are some prevailing theories as to the mechanism. The theories can be divided between antigen-dependent and antigen-independent categories.[5]
Antigen-dependent theories
These theories consider a specific combination of antigen peptide sequence and the binding groove (B pocket) of HLA-B27 (which will have different properties to the other HLA-B alleles). The arthritogenic peptide hypothesis suggests that HLA-B27 has a unique ability to bind antigens from a microorganism that trigger a CD8 T-cell response that then cross-reacts with a HLA-B27/self-peptide pair. Furthermore, it has been shown that HLA-B27 can bind peptides at the cell surface.[6] The molecular mimicry hypothesis is similar, however it suggests that cross reactivity between some bacterial antigens and self peptide can break tolerance and lead to autoimmunity.[5]
Antigen-independent theories
These theories refer to the unusual biochemical properties that HLA-B27 has. The misfolding hypothesis suggests that slow folding during HLA-B27's tertiary structure folding and association with β2 microglobulin causes the protein to be misfolded, therefore initiating the unfolded protein response (UPR) - a pro-inflammatory endoplasmic reticulum (ER) stress response. However, although this mechanism has been demonstrated both in vitro and in animals, there is little evidence of its occurrence in human spondyloarthritis.[6] Also, the HLA-B27 heavy chain homodimer formation hypothesis suggests that B27 heavy chains tend to dimerise and accumulate in the ER, once again, initiating the UPR.[5] Alternatively, cell surface B27 heavy chains and dimers can bind to regulatory immune receptors such as members of the killer cell immunoglobulin-like receptor family, promoting the survival and differentiation of pro-inflammatory leukocytes in disease.
Associated pathology
In addition to its association with ankylosing spondylitis, HLA-B27 is implicated in other types of seronegative spondyloarthropathy[7] as well, such as reactive arthritis (formerly known as Reiter's Syndrome), certain eye disorders such as acute anterior uveitis and iritis, psoriatic arthritis and ulcerative colitis associated spondyloarthritis. The shared association with HLA-B27 leads to increased clustering of these diseases.[8]
See also
References
- 1 2 3 M. A. Khan (2010). "HLA and spondyloarthropathies". In Narinder K. Mehra. The HLA Complex in Biology and Medicine. New Delhi, India: Jayppee Brothers Medical Publishers. pp. 259–275. ISBN 978-81-8448-870-8.
- ↑ Deeks, S. G., Walker, B. D. Human Immunodeficiency Virus Controllers: Mechanisms of Durable Virus Control in the Absence of Antiretroviral Therapy. Immunity, 2007, 27: 406-416
- ↑ Feldtkeller, Ernst; Muhammad, Khan; van der Heijde, Desiree; van der Linden, Sjef; Braun, Jurgen (2003). "Age at disease onset and diagnosis delay in HLA-B27 negative vs. positive patients with ankylosing spondylitis". Rheumatology International. 23 (2): 61–66.
- ↑ Thomas GP, Brown MA. Genetics and Genomics of Ankylosing Spondylitis. Immunol Rev. 2010; 233:162-180.
- 1 2 3 Hacquard-Bouder, C., Ittah, M., Breban, M. Animal models of HLA-B27 associated diseases:new outcoumes. Joint Bone Spine, 2005, 73: 132-138
- 1 2 Bowness, Paul (2015-01-01). "HLA-B27". Annual Review of Immunology. 33: 29–48. doi:10.1146/annurev-immunol-032414-112110. ISSN 1545-3278. PMID 25861975.
- ↑ Elizabeth D Agabegi; Agabegi, Steven S. (2008). Step-Up to Medicine (Step-Up Series). Hagerstwon, MD: Lippincott Williams & Wilkins. ISBN 0-7817-7153-6.
- ↑ Kataria, RK; Brent LH (June 2004). "Spondyloarthropathies". American Family Physician. 69 (12): 2853–2860. PMID 15222650.
External links
- HLA-B27 Syndromes at eMedicine by A. Luisa Di Lorenzo, MBBCh
- Bowness P (2002). "HLA B27 in health and disease: a double-edged sword?". Rheumatology (Oxford). 41 (8): 857–68. doi:10.1093/rheumatology/41.8.857. PMID 12154202.
- Online Mendelian Inheritance in Man (OMIM) 142830
- HLA-B27 at the US National Library of Medicine Medical Subject Headings (MeSH)
- BASDAI and Ankylosing Spondylitis