Gonadotropin-releasing hormone antagonist
| Gonadotropin-releasing hormone antagonist | |
|---|---|
| Drug class | |
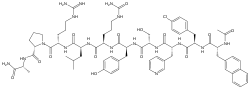 Cetrorelix, one of the most widely used GnRH antagonists. | |
| Class identifiers | |
| Synonyms | GnRH receptor antagonists; GnRH blockers; GnRH inhibitors; Antigonadotropins |
| Use | Infertility; Prostate cancer; Precocious puberty; Breast cancer; Endometriosis; Uterine fibroids; Transgender people |
| Biological target | GnRH receptor |
| Chemical class | Peptides; Non-peptides |
| In Wikidata | |
Gonadotropin-releasing hormone antagonists (GnRH antagonists) are a class of medications that antagonize the gonadotropin-releasing hormone receptor (GnRH receptor) and thus the action of gonadotropin-releasing hormone (GnRH). They are used in the treatment of prostate cancer, endometriosis, uterine fibroids, female infertility in assisted reproduction, and for other indications.
Some GnRH antagonists, such as cetrorelix, are similar in structure to natural GnRH (a hormone made by neurons in the hypothalamus) but that have an antagonistic effect, while other GnRH antagonists, such as elagolix, are non-peptide and small-molecule compounds. GnRH antagonists compete with natural GnRH for binding to GnRH receptors, thus decreasing or blocking GnRH action in the body.
Medical uses
Prostate cancer
Testosterone promotes growth of many prostate tumors and therefore reducing circulating testosterone to very low (castration) levels is often the treatment goal in the management of men with advanced prostate cancer. GnRH antagonists are used to provide fast suppression of testosterone without the surge in testosterone levels that is seen when treating patients with GnRH agonists.[1] In patients with advanced disease, this surge in testosterone can lead to a flare-up of the tumour, which can precipitate a range of clinical symptoms such as bone pain, urethral obstruction, and spinal cord compression. Drug agencies have issued warnings regarding this phenomenon in the prescribing information for GnRH agonists. As testosterone surge does not occur with GnRH antagonists, there is no need for patients to receive an antiandrogen as flare protection during prostate cancer treatment. GnRH agonists also induce an increase in testosterone levels after each reinjection of the drug – a phenomenon that does not occur with GnRH antagonists.
The reduction in testosterone levels that occurs during GnRH antagonist therapy subsequently reduces the size of the prostate cancer. This in turn results in a reduction in prostate-specific antigen (PSA) levels in the patient’s blood and so measuring PSA levels is a way to monitor how patients with prostate cancer are responding to treatment. GnRH antagonists have an immediate onset of action leading to a fast and profound suppression of testosterone and are therefore especially valuable in the treatment of patients with prostate cancer, where fast control of disease is needed.
The GnRH antagonist abarelix was withdrawn from the United States market in 2005 and is now only marketed in Germany for use in patients with symptomatic prostate cancer. Degarelix is a GnRH antagonist that is approved for use in patients with advanced hormone-sensitive prostate cancer throughout Europe and also in the United States.[2]
Fertility treatment
GnRH antagonists are also used for short periods in the prevention of premature LH surge and endogenous ovulation in patients undergoing ovarian hyperstimulation with FSH in preparation for in-vitro fertilization (IVF).[3][4][5] Typically they are administered in the mid-follicular phase in stimulated cycles after administration of gonadotropins and prior to the administration of hCG – which is given to stimulate ovulation. This protocol is likely beneficial in women expected to be hyper-responders, and probably also those expected to be poor responders to ovarian hyperstimulation.[6] The GnRH antagonists that are currently licensed for use in fertility treatment are cetrorelix and ganirelix.
Endometriosis
Elagolix is indicated for moderate to severe endometriosis pain.
Other uses
GnRH antagonists are being investigated in the treatment of women with hormone-sensitive breast cancer and some benign disorders such as uterine fibroids.[7][8] In men, they are being investigated in the treatment of benign prostatic hyperplasia[9] and also as potential contraceptive agents.[10]
Available forms
Currently approved GnRH antagonists include the peptide molecules abarelix, cetrorelix, degarelix, and ganirelix and the small-molecule compound elagolix. GnRH antagonists are administered by subcutaneous injection (cetrorelix, degarelix, ganirelix), by intramuscular injection (abarelix), or by oral administration (elagolix).
Non-peptide and orally-active GnRH antagonists like elagolix that are in development include relugolix and linzagolix.[11]
| Name | Brand/code name(s) | Approved/intended uses | Type | Route(s) | Launch/status* | Hits |
|---|---|---|---|---|---|---|
| Abarelix | Plenaxis | Prostate cancer | Peptide | IM | 2003 | 116,000 |
| Cetrorelix | Cetrotide | Female infertility (assisted reproduction) | Peptide | SC | 2000 | 134,000 |
| Degarelix | Firmagon | Prostate cancer | Peptide | SC | 2008 | 291,000 |
| Elagolix | Orilissa | Endometriosis; Uterine fibroids | Non-peptide | Oral | 2018 | 126,000 |
| Ganirelix | Orgalutran | Female infertility (assisted reproduction) | Peptide | SC | 2000 | 134,000 |
| Linzagolix | KLH-2109; OBE-2109 | Endometriosis; Uterine fibroids | Non-peptide | Oral | Phase III[12] | 9,730 |
| Relugolix | RVT-601; TAK-385 | Endometriosis; Prostate cancer; Uterine fibroids | Non-peptide | Oral | Pre-registration[13] | 44,900 |
| Launch/status = Launch year or developmental status (as of February 2018). Hits = Google Search hits (as of February 2018). | ||||||
Side effects
As with all hormonal therapies, GnRH antagonists are commonly associated with hormonal side effects such as hot flushes, headache, nausea and weight gain.[14][15][16] When used in fertility treatment they can also be associated with abdominal pain and ovarian hyperstimulation.[14][16] Subcutaneously administered agents are also associated with injection-site reactions[15][17] and abarelix (neither of these being GnRH agonists, but instead being antagonists) has been linked with immediate-onset systemic allergic reactions.[18]
Pharmacology
GnRH antagonists competitively and reversibly bind to GnRH receptors in the pituitary gland, blocking the release of luteinizing hormone (LH) and follicle-stimulating hormone (FSH) from the anterior pituitary.[19][20] In men, the reduction in LH subsequently leads to rapid suppression of testosterone production in the testes; in women it leads to suppression of estradiol and progesterone production from the ovaries. GnRH antagonists are able to abolish gonadal sex hormone production and to suppress sex hormone levels into the castrate range, or by approximately 95%.
Unlike the GnRH agonists, which cause an initial stimulation of the hypothalamic–pituitary–gonadal axis (HPG axis) that leads to a surge in testosterone or estrogen levels, GnRH antagonists have an immediate onset of action and rapidly reduce sex hormone levels without an initial surge.[1][21]
Chemistry
GnRH antagonists include peptides such as cetrorelix and non-peptide and small-molecule compounds such as elagolix. Peptide GnRH antagonists are GnRH analogues.
| Compound | Amino acid sequence | Marketed |
|---|---|---|
| Cetrorelix | Ac-D-Nal-D-Cpa-D-Pal-Ser-Tyr-D-Cit-Leu-Arg-Pro-D-Ala-NH2 | Yes |
| Abarelix | Ac-D-Nal-D-Cpa-D-Pal-Ser-N-MeTyr-D-Asn-Leu-Lys(iPr)-Pro-D-Ala-NH2 | Yes |
| Ganirelix | Ac-D-Nal-D-Cpa-D-Pal-Ser-Tyr-D-hArg(Et)2-Leu-hArg(Et)2-Pro-D-Ala-NH2 | Yes |
| Degarelix | Ac-D-Nal-D-Cpa-D-Pal-Ser-Aph(Hor)-D-Aph(Cba)-Leu-Lys(iPr)-Pro-D-Ala-NH2 | Yes |
| Teverelix | Ac-D-Nal-D-Cpa-D-Pal-Ser-Tyr-D-hCit-Leu-Lys(iPr)-Pro-D-Ala-NH2 | No |
| Ozarelix | Ac-D-Nal-D-Cpa-D-Pal-Ser-N-MeTyr-D-hCit-Nle-Arg-Pro-D-Ala-NH2 | No |
| Ornirelix | Ac-D-Nal-D-Cpa-D-Pal-Ser-Lys(Pic)-D-Orn(6Anic)-Leu-Lys(iPr)-Pro-D-Ala-NH2 | No |
| Iturelix | Ac-D-Nal-D-Cpa-D-Pal-Ser-Lys(Nic)-D-Lys(Nic)-Leu-Lys(iPr)-Pro-D-Ala-NH2 | No |
| Acyline | Ac-D-Nal-D-Cpa-D-Pal-Ser-Aph(Ac)-D-Aph(Ac)-Leu-Lys(iPr)-Pro-D-Ala-NH2 | No |
| Azaline B | Ac-D-Nal-D-Cpa-D-Pal-Ser-Aph(Atz)-D-Aph(Atz)-Leu-Lys(iPr)-Pro-D-Ala-NH2 | No |
See also
References
- 1 2 Van Poppel H, Nilsson S (June 2008). Testosterone surge: rationale for gonadotropin-releasing hormone blockers? Urology 71: 1001-1006.
- ↑ Anderson J (May 2009). Degarelix: a novel gonadotropin-releasing hormone blocker for the treatment of prostate cancer. Future Oncol. 5: 433-443.
- ↑ Bodri D, Vernaeve V, Guillen JJ, et al (September 2006). Comparison between a GnRH antagonist and a GnRH agonist flare-up protocol in oocyte donors: a randomized clinical trial. Hum. Reprod. 21: 2246-2251.
- ↑ Lambalk CB, Leader A, Olivennes F, et al (March 2006). Treatment with the GnRH antagonist ganirelix prevents premature LH rises and luteinization in stimulated intrauterine insemination: results of a double-blind, placebo-controlled, multicentre trial. Hum. Reprod. 21: 632-639.
- ↑ Lee TH, Lin YH, Seow KM, et al (July 2008). Effectiveness of cetrorelix for the prevention of premature luteinizing hormone surge during controlled ovarian stimulation using letrozole and gonadotropins: a randomized trial. Fertil. Steril. 90: 113-120.
- ↑ La Marca, A.; Sunkara, S. K. (2013). "Individualization of controlled ovarian stimulation in IVF using ovarian reserve markers: From theory to practice". Human Reproduction Update. 20 (1): 124–40. doi:10.1093/humupd/dmt037. PMID 24077980.
- ↑ Engel JB, Audebert A, Frydman R, et al (October 2007). Presurgical short term treatment of uterine fibroids with different doses of cetrorelix acetate: a double-blind, placebo-controlled multicenter study. Eur. J. Obstet. Gynecol. Reprod. Biol. 134: 225-232.
- ↑ Weiss JM, Diedrich K, Ludwig M (2002). Gonadotropin-releasing hormone antagonists: pharmacology and clinical use in women. Treat. Endocrinol. 1: 281-291.
- ↑ Debruyne F, Gres AA, Arustamov DL (July 2008). Placebo-controlled dose-ranging phase 2 study of subcutaneously administered LHRH antagonist cetrorelix in patients with symptomatic benign prostatic hyperplasia. Eur. Urol. 54: 170-177.
- ↑ Amory JK (March 2007). Contraceptive developments for men. Drugs Today (Barc.) 43: 179-192.
- ↑ Ezzati, Mohammad; Carr, Bruce R (2015). "Elagolix, a novel, orally bioavailable GnRH antagonist under investigation for the treatment of endometriosis-related pain". Women's Health. 11 (1): 19–28. doi:10.2217/whe.14.68. ISSN 1745-5057.
- ↑ http://adisinsight.springer.com/drugs/800032710
- ↑ http://adisinsight.springer.com/drugs/800028257
- 1 2 Serono. Cetrotide prescribing information 2009. Accessed 18-6-2009.
- 1 2 Degarelix US prescribing information 2008. Accessed 28-4-2009.
- 1 2 Organon. Ganirelix acetate prescribing information 2009. Accessed 18-6-2009.
- ↑ Klotz L, Boccon-Gibod L, Shore ND, et al (December 2008). The efficacy and safety of degarelix: a 12-month, comparative, randomized, open-label, parallel-group phase III study in patients with prostate cancer. BJU. Int. 102: 1531-1538.
- ↑ Debruyne F, Bhat G, Garnick MB (December 2006). Abarelix for injectable suspension: first-in-class gonadotropin-releasing hormone antagonist for prostate cancer. Future Oncol. 2: 677-696.
- ↑ Broqua P, Riviere PJ, Conn PM, et al (April 2002). Pharmacological profile of a new, potent, and long-acting gonadotropin-releasing hormone antagonist: degarelix. J. Pharmacol. Exp. Ther. 301: 95-102.
- ↑ Engel JB, Schally AV (February 2007). Drug Insight: clinical use of agonists and antagonists of luteinizing-hormone-releasing hormone. Nat. Clin. Pract. Endocrinol. Metab.: 3: 157-167.
- ↑ Gustofson RL, Segars JH, Larsen FW (November 2006). Ganirelix acetate causes a rapid reduction in estradiol levels without adversely affecting oocyte maturation in women pretreated with leuprolide acetate who are at risk of ovarian hyperstimulation syndrome. Hum. Reprod. 21: 2830-2837.
- ↑ Mezo G, Manea M (December 2009). "Luteinizing hormone-releasing hormone antagonists". Expert Opin Ther Pat. 19 (12): 1771–85. doi:10.1517/13543770903410237. PMID 19939192.
External links
- Degarelix Product website
- Fertility Lifelines website
- Fertility Treatments website
- Fertility Information website