HIV/AIDS in Nepal
Nepal's first cases of HIV/AIDS were reported in 1988 and the disease has primarily been transmitted by intravenous drug use and unprotected sex. Among the two, HIV epidemic is largely attributed to sexual transmissions which account for more than 85% of the total new HIV infections.Available data indicate that there was a sharp increase in the number of new infections starting in 1996, coinciding with the outbreak of civil unrest. The infection rate of HIV/AIDS in Nepal among the adult population is estimated to be below the 1 percent threshold which is considered "generalized and severe". However, the prevalence rate masks a concentrated epidemic among at-risk populations such as female sex workers (FSWs), male sex workers (MSWs), injecting drug users (IDUs), men who have sex with men (MSM), Transgender Groups (TG), migrants and Male Labor Migrants(MLMs) as well as their spouses. Cultural factors have also been shown to play a significant role in the spread of HIV and AIDS in Nepal. Some of these cultural factors are related with social taboos which creates challenges for open discussions regarding sex and sexual habits, as do denial, stigma, and discrimination that surround HIV and AIDS. Other factors such as poverty, low levels of education and literacy, political instability combined with gender inequality make the tasks challenging.[1][2]
Prevalence
As of December 2007, the Government of Nepal reported 1,610 cases of AIDS and 10,546 HIV infections, which has grown to 13,000 infections by World AIDS Day 2008.[3] UNAIDS estimates from 2007 indicate that approximately 75,000 people in Nepal are HIV-positive, including all age groups. The Government of Nepal's National Center for AIDS & STD Control (NCASC) estimated that number to be closer to 70,000 in December 2007. In a study from 2014, an overall national HIV prevalence was 0.20% (adult male 0.28%, adult female 0.13%). According to UNAIDS, by the end of 2015, the number of people living with HIV was 39,000 [34,000 - 46,000][4] NCASC (2010) reports that estimated number of HIV infections by risk groups is 59,984[5][2]
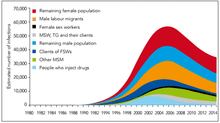
The epidemic in Nepal is driven by IDUs, migrants, sex workers and their clients, and MSM. Results from the 2007 Integrated Bio-Behavioral Surveillance Study (IBBS) among IDUs in Kathmandu, Pokhara, and East and West Terai indicate that the highest prevalence rates have been found among urban IDUs, 6.8 percent to 34.7 percent of whom are HIV-positive, depending on location. In terms of absolute numbers, Nepal's 1.5 million to 2 million labor migrants account for the majority of Nepal’s HIV-positive population. In one subgroup, 2.8 percent of migrants returning from Mumbai, India, were infected with HIV, according to the 2006 IBBS among migrants.[4]
As of 2007, HIV prevalence among female sex workers and their clients was less than 2 percent and 1 percent, respectively, and 3.3 percent among urban-based MSM. HIV and AIDS case reporting by the NCASC reports HIV infections to be more common among men than women, as well as in urban areas and the far western region of Nepal, where migrant labor is more common. According to Nepal's 2007 United Nations General Assembly Special Session (UNGASS) report, labor migrants make up 41 percent of the total known HIV infections in Nepal, followed by clients of sex workers (15.5 percent) and IDUs (10.2 percent).[4]
Migrants have become so vulnerable to infection due to uncertainty about their immigration status.[6] India and Nepal have an open borders policy, whereby Nepalese citizens have the same rights as Indians to live and work in India and vice versa.[6] However, there is low awareness of this agreement and as a result many migrants avoid any contact with the state, including health services. There are also many cases of human trafficking for the sex trade. Not only are all sex-workers at risk, but Nepalese sex workers are often isolated from peers due to language barriers. Those peer network are important for providing information about prevention.[6]
The annual new infection in 2014 is estimated at 1,493 and is expected to decline by 899 by 2020. An estimated number of 2,576 deaths were caused by AIDS in 2014, lower compared to estimated 3,362 deaths in 2013 which is, largely due to increased access to treatments. While the most recent data demonstrate a stabilizing of the epidemic and a downward trend in seroprevalence among several of the key high-risk groups, a number of issues pose continued challenges for Nepal. Many sex workers are also IDUs, migrants, or both, increasing the spread of HIV among at-risk groups. A large portion of men who purchase sex are also married, making them potential conduits for HIV to bridge to the general population. Poverty, low levels of education, illiteracy, gender inequalities, marginalization of at-risk groups, and stigma and discrimination compound the epidemic's effects. Unsafe sex and drug injection practices, civil conflict, internal and external mobility, and limited adequate health care delivery multiply the difficulties of addressing HIV/AIDS. Moreover, existing care and support services are already overwhelmed as increasing numbers of HIV-infected individuals become sick with AIDS.[4][2]
Street children are also one of the most vulnerable groups. The UNICEF report, "Increasing Vulnerability of Children in Nepal", estimates the number of children orphaned by HIV/AIDS to be more than 13,000. The national estimate of children 0 to 14 years of age infected by HIV is 2,500 (2007).[4]
Nepal has a high tuberculosis (TB) burden, with 81 new cases per 100,000 people in 2005, according to the World Health Organization. HIV infects 3.1 percent of adult TB patients, and HIV-TB co-infections complicate treatment and care for both diseases.[4]
Risk Factors
- Injecting Drug Use:
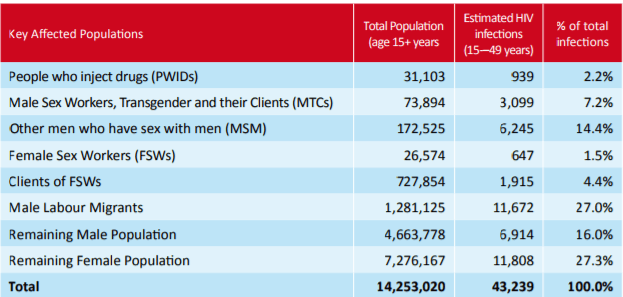
Nepal was the first developing country to establish harm reduction program with needle exchange for IDUs. However, due to limited resources the coverage of this program was minimal which caused limited effect on prevention of HIV transmissions. In 2011, the estimated number of IDUs in Nepal was between 30,155 and 33,742 including 939 IDUs who are living with HIV or AIDS. The highway districts, border towns and Kathmandu Valley have highest number of IDUs where 30% of all people living with HIV/AIDS are IDUs. In 2011, within the Kathmandu valley, HIV prevalence among IDUs was 6.3% which is significantly lower than 20.7% in 2009. Such a decline in prevalence, to some extent can be attributed to improving behavioral indicators measured by three successive rounds of integrated biological and behavioral surveys (IBBS). [7]
- Trafficking of female sex workers:
There are between 24,649 - 28,359 female sex workers in Nepal with an estimated HIV prevalence of 1.69%. In the Kathmandu valley alone, the HIV infection rate among street-based sex workers is 4.2%. FSWs in Nepal have limited or no access to information about reproductive health and safe sex practices because of their highly marginalized status. Due to cultural, social and economic constraints, it becomes difficult for FSWs to negotiate condom usage with their clients or obtaining health services and legal counseling. Their clients consist of transport workers, members of police force or military, and migrant workers who do not use condoms which constitutes 60% of their client base. Trafficking of Nepalese girls and women into commercial sex work in India has been a major issue to HIV.50% of Nepalese sex workers in Mumbai brothels are HIV positive(FHI 2004).
- High rates of migration and mobility:
Migration for work amounts to an internal and external migration of about 1.5 to 2 million people. Such migration ranges from seasonal migration to long-term migration. Migration for work is integral for economic survival of many households in rural and urban areas. As a migrant in foreign nations, they are not regulated by traditional social structures and customs which can lead to unsafe sexual practices, such as having multiple sexual partners and buying sex. HIV prevalence in migrants returning from Mumbai is suggested to be nearly 8 percent, according to a 2002 study. As of 2011, 27% of estimated HIV infections in Nepal are of male labor migrants.[7]
National response
The NCASC coordinates Nepal's response to the HIV/AIDS epidemic. In 1992, the Government of Nepal founded the National AIDS Coordination Committee to lead the multisectoral response to HIV/AIDS and followed with the establishment of the National AIDS Council to oversee the Committee's efforts. However, both the Council and the Committee have been ineffective, in part because of civil strife.[4]
Despite this fact, substantial progress has been made with respect to national commitment and a strengthened response to address the HIV/AIDS epidemic in the country. HIV and AIDS have been recognized as a priority in the new interim three-year development plan. The national program is implemented under one national HIV/AIDS action plan framework. A national monitoring and evaluation system has been developed, and the Government of Nepal has taken initial steps toward establishing a semi-autonomous coordination body for HIV and AIDS. There is strong civil society engagement in the response.[4]
Given the nature of the epidemic in Nepal, most of the national initiatives have focused on leadership, partnerships and the involvement of civil society for prevention, care, and support for its most-at-risk populations. From 2003, the NCASC implemented the HIV/AIDS Operational Plan based on the National Strategy 2002–2006. Currently, the HIV/AIDS activities are shaped by the second National HIV/AIDS Strategy 2007–2011, and implementation is coordinated under the 2006–2008 National Action Plan, which has the following priorities:
- Preventing the spread of sexually transmitted infections (STIs) and HIV infection among at-risk groups;
- Ensuring universal access to quality treatment, diagnostics, care, and support services for infected, affected, and vulnerable groups;
- Ensuring a comprehensive and well-implemented legal framework on HIV/AIDS promoting human rights and establishing HIV/AIDS as a development agenda;
- Enhancing leadership and management at national and local levels for an effective response to HIV/AIDS;
- Using strategic information to guide planning and implementation for an improved effective response; and
- Achieving sustainable financing and effective utilization of funds.[4]
The vision of the national strategy is to expand the number of partners involved in the national response and to increase the effectiveness of Nepal's response. It also emphasizes prevention as key for an effective response to the epidemic, particularly in areas with high levels of out-migration. The strategy includes care and support for people infected and affected by HIV/AIDS while recognizing the contribution of care and support to effective prevention. It also recognizes the importance of accurately tracking the epidemic to monitor the effectiveness of interventions.[4]
Nepal's political instability has resulted in nominal government support for national HIV and AIDS programs. Therefore, most HIV/AIDS activities are funded by external development partners. Antiretroviral treatment (ART) coverage has increased from no free or publicly available treatment three years ago to 13 percent of those estimated to need ART accessing free treatment. ART drugs are provided through a grant from The Global Fund to Fight AIDS, Tuberculosis and Malaria. While there is a need to expand services further, several organizations provide community care and support services.[4]
According to National Center for AIDS and STD Control, at present, Nepal has 67 Antiretroviral treatment (ART) sites. ART service was first started from the Central development region and the Mid-western region simultaneously in 2004. In the Central Development region, the ART service was started from Sukraraj Tropical & Infectious Disease Control Hospital located in Teku, Kathmandu and in the Mid-western region, the ART services was started from the Bheri Zonal Hospital located in Nepalgunj, Banke. Currently, there 19 Antiretroviral treatment (ART) sites in Central development region. Similarly, there are 10, 12, 15 and 11 Antiretroviral treatment (ART) sites in Mid-Western development region, Eastern development region, Western development region and Far-Western development region respectively.[8]
Nepal receives assistance from several international donor organizations, including The Global Fund and Great Britain's Department for International Development. The Global Fund approved a second-round grant in 2003 to support HIV/AIDS prevention among labor migrants and young people and to care for HIV-infected individuals. Nepal was also approved for a seventh-round grant in 2007 that will focus on labor migrants and target gaps in services for MSM and IDUs.[4]
Non Government Organisations (NGOs) in Nepal
NGOs operating in Nepal must be registered with the Social Welfare Council. The number of registered NGOs in Nepal is significant. The various NGOs provide a range of services within the communities served including Care and Support, Health Education, Advocacy, Income Generation etc.[9]
On 28 September 2008 a number of NGOs met with representatives from the Constituent Assembly in an interaction programme organized by Naulo Ghumti Nepal, a local NGO. At this meeting Rabindra Prasad Adhikari acknowledged that an effective response to HIV has to be a joint response between the Government and NGOs operating in Nepal. After this event, an informal caucus of four parliamentarians namely Sapana Pradhan Malla, RajKaji Tamu, Dhanraj Gurung, and Rabindra Adhikari was formed. The group was requested to act as a focal point of HIV in the parliament.[10]
See also
Further reading
Beine, David. 2003. Ensnared by AIDS: Cultural Contexts of HIV/AIDS in Nepal. Kathmandu, Nepal: Mandala Book Point.
Beine, David. 2002. “HIV/AIDS in Nepal: The Making of a Cultural Model.” Journal of the Center for Nepal Asian Studies 29(2): 275-310.
References
- Beine, David. 2003. Ensnared by AIDS: Cultural Contexts of HIV/AIDS in Nepal. Kathmandu, Nepal: Mandala Book Point.
- "Country Progress Report Nepal".UNAID.
- Nearly 13,000, The Hindu, "Nearly 13,000 HIV/AIDS cases recorded in Nepal", December 8, 2008, retrieved April 28, 2011.
- "Health Profile: Nepal" Archived 2008-08-17 at the Wayback Machine. United States Agency for International Development (March 2008). Accessed August 25, 2008.

- Fiona Samuels and Sanju Wagle 2011. Population mobility and HIV and AIDS: review of laws, policies and treaties between Bangladesh, Nepal and India. London: Overseas Development Institute
- "HIV/AIDS in Nepal"
- VSO Nepal
- Noble Voice, October 2008 issue, a quarterly newsletter of Naulo Ghumti Nepal and different governmental and non govern mental institution are involved in it. We have Ravi Pd. Dangol who is working there in the management of HIV AIDS in Nepal.
| Sovereign states |
|
|---|---|
| States with limited recognition |
|
| Dependencies and other territories |
|
| |