Tonsillectomy
| Tonsillectomy | |
|---|---|
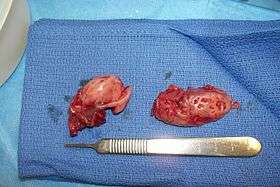 Cryptic tonsils immediately following surgical removal (bilateral tonsillectomy). | |
| ICD-9-CM | 28.2-28.3 |
| MeSH | D014068 |
| MedlinePlus | 003013 |
Tonsillectomy is a surgical procedure in which both palatine tonsils (hereafter called "tonsils") are removed from a recess in the side of the pharynx called the tonsillar fossa. The procedure is performed in response to repeated occurrence of acute tonsillitis, sleep surgery for obstructive sleep apnea, nasal airway obstruction, diphtheria carrier state, snoring, or peritonsillar abscess. For children, tonsillectomy is usually combined with an adenoidectomy, which is the removal of the adenoid (also known as the "pharyngeal tonsil" or "nasopharyngeal tonsil"). The combination of these two procedures is called an "adenotonsillectomy" or "T&A". Adenoidectomy is uncommon in adults in whom the adenoid is much smaller than in children and rarely causes problems. Although tonsillectomy is nowadays performed much less frequently than in the 1950s through 1970s, it remains a common surgical procedure in children in the United States and many other western countries. However, tonsillectomy is still a controversial surgery as its benefits seem to be only modest and temporary in most cases, there are recognised hazards associated with the operation and there are several indications that tonsillectomy may compromise the immune system in the long run, especially when performed at a young age.
History
Tonsillectomies have been practiced for over 2,000 years, with varying popularity over the centuries.[1] The procedure is claimed in some books as "Hindu medicine" about 1000 BCE (non-evidence based literature). Others refer to it as cleaning of tonsil using the nail of the index finger. Roughly a millennium later the Roman aristocrat Aulus Cornelius Celsus (25 BCE – 50 CE) described a procedure whereby using the finger (or a blunt hook if necessary), the tonsil was separated from the neighboring tissue before being cut out.[1] Galen (121–200 CE) was the first to advocate the use of the surgical instrument known as the snare, a practice that was to become common until Aetius (490 CE) recommended partial removal of the tonsil, writing "Those who extirpate the entire tonsil remove, at the same time, structures that are perfectly healthy, and, in this way, give rise to serious Hæmorrhage".[1] In the 7th century Paulus Aegineta (625–690) described a detailed procedure for tonsillectomy, including dealing with the inevitable post-operative bleeding. 1,200 years pass before the procedure is described again with such precision and detail.[1]
The Middle Ages saw tonsillectomy fall into disfavor; Ambroise Pare (1509) wrote it to be "a bad operation" and suggested a procedure that involved gradual strangulation with a ligature. This method was not popular with the patients due to the immense pain it caused and the infection that usually followed. Scottish physician Peter Lowe in 1600 summarized the three methods in use at the time, including the snare, the ligature, and the excision.[1] At the time, the function of the tonsils was thought to be absorption of secretions from the nose; it was assumed that removal of large amounts of tonsillar tissue would interfere with the ability to remove these secretions, causing them to accumulate in the larynx, resulting in hoarseness. For this reason, physicians like Dionis (1672) and Lorenz Heister censured the procedure.

In 1828, physician Philip Syng Physick modified an existing instrument originally designed by Benjamin Bell for removing the uvula; the instrument, known as the tonsil guillotine (and later as a tonsillotome), became the standard instrument for tonsil removal for over 80 years.[1] By 1897, it became more common to perform complete rather than partial removal of the tonsil after American physician Ballenger noted that partial removal failed to completely alleviate symptoms in a majority of cases. His results using a technique involving removal of the tonsil with a scalpel and forceps were much better than partial removal; tonsillectomy using the guillotine eventually fell out of favor in America.[1]
Medical uses

Tonsillectomy may be indicated when the patient experiences recurrent infections of acute tonsillitis. As the size of tonsils reaches its maximum at 3 years of age and then regresses gradually, tonsillectomy is usually delayed unless the frequency of infection necessitates it absolutely. The number prompting tonsillectomy varies with the severity of the episodes. One case, even severe, is generally not enough for most surgeons to decide tonsillectomy is necessary. Paradise in 1983 defined recurrent tonsillitis warranting surgery by the attack frequency standard as
Seven or more in a year, five or more per year for two years, or three or more per year for three years. These are the absolute indications for tonsillectomy.[2]
According to the 2012 guidelines of the American Academy of Otolaryngology & Head and Neck Surgery (AAO-HNS), tonsillectomy is indicated as follows:
Clinicians may recommend tonsillectomy for recurrent throat infection with a frequency of at least 7 episodes in the past year or at least 5 episodes per year for 2 years or at least 3 episodes per year for 3 years with documentation in the medical record for each episode of sore throat and one or more of the following: temperature >38.3 °C, cervical adenopathy, tonsillar exudates, or positive test for Group A Beta- hemolytic strep.[3]
Tonsillectomy is also sometimes performed on those who suffer chronically from tonsilloliths.[4]
Most recently, the American Academy of Otolaryngology–Head and Neck Surgery Foundation has published clinical practice guidelines.[5][6] The panel made a strong recommendation for the following:
- Watchful waiting for recurrent throat infection if there have been fewer than 7 episodes in the past year or fewer than 5 episodes per year in the past 2 years or fewer than 3 episodes per year in the past 3 years;
- Assessing the child with recurrent throat infection who does not meet criteria in statement 2 for modifying factors that may nonetheless favor tonsillectomy, which may include but are not limited to multiple antibiotic allergy/intolerance, periodic fever, aphthous stomatitis, pharyngitis and adenitis, or history of peritonsillar abscess;
- Asking caregivers of children with sleep-disordered breathing and tonsil hypertrophy about comorbid conditions that might improve after tonsillectomy, including growth retardation, poor school performance, enuresis, and behavioral problems;
- Counseling caregivers about tonsillectomy as a means to improve health in children with abnormal polysomnography who also have tonsil hypertrophy and sleep-disordered breathing;
- Counseling caregivers that sleep-disordered breathing may persist or recur after tonsillectomy and may require further management;
- Advocating for pain management after tonsillectomy and educating caregivers about the importance of managing and reassessing pain; and
- Clinicians who perform tonsillectomy should determine their rate of primary and secondary post-tonsillectomy hemorrhage at least annually.
Effectiveness
The scientific evidence indicates that tonsillectomy is only modestly effective at reducing the frequency and severity of sore throats, and does not get rid of sore throats altogether, probably because most sore throats are not caused by infected tonsils.[7][8][9][10][11][12] Benefits also appear to only last for one or two years after surgery as children usually outgrow tonsil related diseases (which is why children are sometimes removed from the waiting list), making surgery seem more effective than it really is.[13][14][15] Some patients do experience long term results, although more information and studies need to be done to portray the full picture on the matter.[16] Most parents and patients are satisfied with the results of tonsillectomy, but it should be kept in mind that their views are prone to bias.[15]
This raises questions about which children benefit enough to justify undertaking the operation.[17] Even in children who meet strict criteria indicating that they are severely affected by sore throats, the evidence indicates that there is only a short term benefit.[18] Without tonsillectomy a child who meets these strict criteria will probably have 6 sore throats in the next two years and one who has surgery will probably have 3 sore throats in the next two years. After two years there is little difference in the frequency of sore throats whether or not the child has surgery.[14] Children with undocumented sore throats or sore throats that are not as severe do not appear to suffer from as many sore throats in subsequent years and therefore tonsillectomy is not worthwhile.[9][19]
The strict criteria are that children should have experienced: - 7 documented sore throats in the previous year, - or 5 each year in the two previous years, - or 3 each year in the three previous years and that sore throats should include documented evidence of enlarged lymph glands, or raised temperature, or positive throat swabs (demonstrating Streptococcal infection) or pus seen on the tonsils.
The term "sore throat" is preferred to "throat infection" or "tonsillitis" because without undertaking throat swabs, doctors cannot reliably distinguish between sore throats caused by infection and those due to other causes. Furthermore the same patient may be described as suffering from "tonsillitis" or "sore throat" by another, therefore the use of one term rather than the other is as dependent on the doctor as well as the patient, making it an unreliable reason for undertaking surgery.
Many tonsillectomies are also undertaken for sleep apnea but for this there is insufficient evidence to say if this is more effective than no surgery.[9][20] Because the effectiveness of tonsillectomy for breathing related problems is not known there are ongoing clinical trials to investigate whether it is effective.[21][22]
Overtreatment with tonsillectomy
There are significant differences in tonsillectomy rates, both between and within countries, indicating that many tonsillectomies may in fact be done without sufficient medical justification.[9][23] (The Dartmouth Atlas of Health Care. Tonsillectomies per 1000 children.) In 2015, tonsillectomy rates in Belgium, Finland and Norway were twice those in the UK but rates in Spain, Italy and Poland were at least a quarter lower. (Eurostat) Childhood tonsillectomy rates are three times higher in the USA than England and are among the highest rates in the world.[9][5]
A 2010 study found that, between 2000 and 2005, the highest regional annual tonsillectomy rate in England was 754 per 100.000, which was more than twice the average of 304 per 100.000 and seven times as high as the lowest one of 102 per 100.000.[24] In 2006, Chief Medical Officer Liam Donaldson revealed that unnecessary tonsillectomies and unnecessary hysterectomies combined cost the British National Health Service 21 million Pounds a year.[25]
The reasons why ENT surgeons remove tonsils are complex and include clinician and patient beliefs about effectiveness. Financial incentives and parental pressure are also believed to play a role.[15][26][27][28][29][30] But there is insufficient scientific evidence from randomised controlled trials to support the use of tonsillectomy for obstructive sleep apnea for recurrent sore throat unless it meets the criteria specified above. There is evidence that tonsillectomy imposes both short term and long term risks on the patient. There is evidence in the United Kingdom, which has a moderately high tonsillectomy rate (lower rates than the US, Germany, Norway, Belgium, higher than Spain or Italy) that most children undergoing tonsillectomy did not benefit from the procedure.[31] And even if children do benefit, then it is still questionable whether the benefits justify both the short and long term risks associated with tonsillectomy.
Many people believe that enlarged tonsils are inflamed (and should therefore be removed), but this is not necessarily the case as the tonsils reach their maximum size between the ages of 5 and 7 and shrink afterwards. Also, enlarged tonsils may very well be the result of disease rather than its cause. Therefore, enlargement is nowadays only considered by surgeons a valid reason for surgery if the tonsils are so large that they are causing airway obstruction.[15]
In the past decades however, tonsillectomies have become less frequent because of awareness that watchful waiting is often preferable to surgery as complaints often spontaneously resolve with age. Furthermore a growing number of doctors believe that the tonsils play an important, if not very important role in the human immune system as the first line of defence. It is generally agreed that even when complaints are severe, not performing surgery will not cause serious complications.[15]
Surgical procedure
For the past 50 years at least, tonsillectomy has been performed by dissecting the tonsil from its surrounding fascia, a so-called total, or extra-capsular tonsillectomy. Problems including pain and bleeding led to a recent resurgence in interest in sub-total tonsillectomy or tonsillotomy, which was popular 60–100 years ago, in an effort to reduce these complications.[32] The generally accepted procedure for 'total' tonsillectomy uses a scalpel and blunt dissection or electrocautery, although harmonic scalpels or lasers have also been used. Bleeding is stopped with electrocautery, ligation by sutures, and the topical use of thrombin, a protein that induces blood clotting.
The main question of importance becomes whether or not the benefits of subtotal tonsillectomy in obstructive sleep apnea are enduring. There have been no randomised controlled trials of long term effectiveness of tonsillectomy for sleep apnea.[9][20]
Methods
The scalpel is the preferred surgical instrument of many ear, nose, and throat specialists. However, there are other techniques and a brief review of each follows:
- Dissection and snare method: Removal of the tonsils by use of a forceps and scissors with a wire loop called a snare was formerly the most common method practiced by otolaryngologists, but has been largely replaced in favor of other techniques. The procedure requires the patient to undergo general anesthesia; the tonsils are completely removed and the remaining tissue surface is cauterized. The patient will leave with minimal post-operative bleeding.
- Electrocautery: Electrocautery uses electrical energy to separate the tonsillar tissue and assists in reducing blood loss through cauterization. Research has shown that the heat of electrocautery (400 °C) may result in thermal injury to surrounding tissue. This may result in more discomfort during the postoperative period.
- Radiofrequency ablation: Monopolar radiofrequency thermal ablation transfers radiofrequency energy to the tonsil tissue through probes inserted in the tonsil. The procedure can be performed in an office (outpatient) setting under light sedation or local anesthesia. After the treatment is performed, scarring occurs within the tonsil causing it to decrease in size over a period of several weeks. The treatment can be performed several times. The advantages of this technique are minimal discomfort, ease of operations, and immediate return to work or school. Tonsillar tissue remains after the procedure but is less prominent. This procedure is recommended for treating enlarged tonsils and not chronic or recurrent tonsillitis.
- Coblation tonsillectomy: This surgical procedure is performed using plasma to remove the tonsils. Coblation technology combines radiofrequency energy and saline to create a plasma field. The plasma field is able to dissociate molecular bonds of target tissue while remaining relatively cool (40-70 °C),[33] which results in minimal or no damage to surrounding healthy tissue. A Coblation tonsillectomy is carried out in an operating room setting, with the patient under general anesthesia. Tonsillectomies are generally performed for two main reasons: tonsillar hypertrophy (enlarged tonsils) and recurrent tonsillitis. It has been claimed that this technique results in less pain, faster healing, and less post operative care.[34] However, review of 21 studies gives conflicting results about levels of pain, and its comparative safety has yet to be confirmed.[35] This technique has been criticized for a higher than expected rate of bleeding presumably due to the low temperature which may be insufficient to seal the divided blood vessels but several papers offer conflicting (some positive, some negative) results. More recent studies of coblation tonsillectomy indicate reduced pain and ostalgia;[36] less intraoperative or postoperative complications;[37] lesser incidence of delayed hemorrhage, more significantly in pediatric populations,[38][39][40] less postoperative pain and early return to daily activities, fewer secondary infections of the tonsil bed and significantly lower rates of secondary hemorrhage.[41] Unlike the electrosurgery procedure, Coblation Tonsillectomy generates significantly lower temperatures on contacted tissue.[42] Long term studies seem to show that surgeons experienced with the technique have very few complications.
- Harmonic scalpel: This medical device uses ultrasonic energy to vibrate its blade at 55kHz. Invisible to the naked eye, the vibration transfers energy to the tissue, providing simultaneous cutting and coagulation. The temperature of the surrounding tissue reaches 80 °C. Proponents of this procedure assert that the end result is precise cutting with minimal thermal damage.
- Thermal Welding: A new technology which uses pure thermal energy to seal and divide the tissue. The absence of thermal spread means that the temperature of surrounding tissue is only 2-3 °C higher than normal body temperature. Clinical papers show patients with minimal post-operative pain (no requirement for narcotic pain-killers), zero edema (swelling) plus almost no incidence of bleeding. Hospitals in the US are advertising this procedure as "Painless Tonsillectomy". Also known as Tissue Welding.
- Carbon dioxide laser: When a laser is used to perform tonsillectomy, it can be under local anaesthetic with anaesthetic spray only, called tonsillotomy (or tonsil resurfacing), or it can be performed under general anaesthetic when it is called intra-capsular tonsillectomy, using an operating microscope for magnification. The carbon dioxide laser in scanning mode is an excellent vapouriser of tissue, and in conjunction with a computerised pattern generator and operating microscope with micromanipulator, it can result in near total removal of tonsil tissue whilst preserving the capsule of the tonsil. This leads to a significantly reduced bleeding and pain rate (Mehta et al www.academia.edu/8734771). The local anaesthetic technique takes around 10 minutes, the general around 20 minutes depending on the size of the tonsils - the bigger they are, the longer it takes. The general anaesthetic operation has a revision rate of 1:50, the local anaesthetic tonsillotomy 1:4.5. This is different from procedures where a laser is used to reduce or resurface the tonsils (e.g. laser cryptolysis). Providing the absence of certain contra-indications such as sensitive gag reflex, LAST can be performed under local anesthetic as an outpatient procedure. A carbon dioxide laser is commonly used, and is swept over each tonsil 8–10 times. The smoke is aspirated out of the mouth to prevent smoke inhalation. Often, more than one procedure is required, each lasting about 20 minutes. Due to the frequent requirement for multiple sessions, this treatment may work out more expensive than a single session tonsillectomy. A degree of patient compliance is required, making it unsuitable for young children and anxious persons, who risk harm if they move during the procedure.[43]
- Microdebrider: The microdebrider is a powered rotary shaving device with continuous suction often used during sinus surgery. It is made up of a cannula or tube, connected to a hand piece, which in turn is connected to a motor with foot control and a suction device. The endoscopic microdebrider is used in performing a partial tonsillectomy, by partially shaving the tonsils. This procedure entails eliminating the obstructive portion of the tonsil while preserving the tonsillar capsule. A natural biologic dressing is left in place over the pharyngeal muscles, preventing injury, inflammation, and infection. The procedure results in less post-operative pain, a more rapid recovery, and perhaps fewer delayed complications. However, the partial tonsillectomy is suggested for enlarged tonsils—not those that incur repeated infections.
Post-operative care
A sore throat will persist approximately two weeks following surgery while pain following the procedure is significant and may necessitate a hospital stay.[44] Recovery can take from 7 to 10 days and proper hydration is very important during this time, since dehydration can increase throat pain, leading to a vicious circle of poor fluid intake.[45][46]
At some point, most commonly 7–11 days after the surgery (but occasionally as long as two weeks (14 days) after), bleeding can occur when scabs begin sloughing off from the surgical sites. The overall risk of bleeding is approximately 1–2%. It is higher in adults, especially males over age 70 and three quarters of bleeding incidents occur on the same day as the surgery.[47] Approximately 3% of adult patients develop significant bleeding at this time which may sometimes require surgical intervention.
Post-operative pain relief is subject to change. Traditionally, pain relief has been provided by relatively mild narcotic analgesics such as Acetaminophen with codeine, for milder pain, and stronger narcotic analgesics for more severe pain. Recently (January 2011), the FDA reduced the recommended total 24-hour dose because of concern about liver toxicity from the Acetominophen component. An alternative is the use of non-steroidal anti-inflammatory agents, themselves giving rise to concerns that their effect on platelets might increase the risk of post-operative bleeding.[48] In turn, this has renewed interest in techniques other than traditional 'extra-capsular excision' in the hope that post-operative pain might be reduced.[49]
Tonsillectomy appears to be more painful in adults than children, although there will be individual variations in response.[50]
Complications
Although tonsillectomy is a relatively safe surgery, serious complications (especially hemorrhage, dehydration and infection) and death do sometimes occur.[9][51][52] Minor complications include voice change and taste disturbance.[53][54][55] Because tonsillectomy takes place under general anaesthesia, there is a small risk of brain damage.[56][57][58] The morbidity rate associated with tonsillectomy s 2% to 4% due to post-operative bleeding; in the US 3.6% of children are readmitted to hospital following tonsillectomy, mainly because of dehydration or bleeding. [9][59] The mortality rate is 1 in 15,000, due to bleeding, airway obstruction, or anesthesia complications.[60]
A single dose of the corticosteroid drug dexamethasone may be given during surgery to prevent post-operative vomiting.[61] A systematic review found that a dose of dexamethasone during surgery can prevent vomiting in one out of every five children who receives the drug.[61] The review also found that these children return to a normal diet more quickly and have less post-operative pain.[61]
A recent study states that tonsillectomies in young children (0 to 7 years) are correlated with weight gain in the years following surgery.[62] However, no causal effect has been established.[63]
Impact on immune system
It remains controversial whether tonsillectomy negatively affects the immune system. However, multiple studies have confirmed correlation between a previous history of tonsillectomy and a wide range of diseases, such as the following:
- Hodgkin's disease[64][65][66][67]
- Non-hodgkin's lymphoma[68]
- Laryngeal cancer[69]
- Esophageal cancer[70]
- Thyroid cancer[71][72]
- Breast cancer[73][74][75]
- Prostate cancer[76]
- Base of tongue cancer[77]
- Leukemia[78][79][80][81]
- Asthma[82][83]
- Pneumonia[83]
- Hay fever[84][85]
- Influenza[83]
- Lung infection[83]
- Kidney infection[83]
- Irritable bowel syndrome[86]
- Crohn's disease[87][88][89][90][91]
- Appendicitis[92][93]
- Heart attack[94]
- Sarcoidosis[95]
- Rheumatoid arthritis[96][97]
- Retropharyngeal and parapharyngeal abscesses[98]
- Otitis media[83][99]
- Multiple sclerosis[100][101][102][103]
- Deep neck infection[104]
- Poliomyelitis[105][106][107][108]
- Recurrent cellulitis[109]
- Primary biliary cholangitis[110][111]
- Rhinosinusitis[83][112]
- Lingual tonsillitis[113][114]
- Pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections[115]
Moreover, other studies have found that tonsillectomy may lead to the following:
- a decrease in levels of serum immunoglobulin[116]
- a permanent decrease in levels of secretory immunoglobulin A[116][117][118]
- a permanent decrease in levels of immunoglobulin G3[119]
- an increased risk of autoimmune disease[83][120]
- a 50% increase in mortality between the age of 18 and 44 (if performed before the age of 7)[121]
- a nine fold increased risk of chronic disease[122]
- an increase in overall cancer risk[72][75]
- a two to three fold increased risk of respiratory diseases (which means that for every five tonsillectomies, one extra case of respiratory disease will be caused) [83]
- an increased risk of infectious diseases[83]
- an increased risk of allergies[83]
Image gallery
 Throat with tonsilloliths.
Throat with tonsilloliths.- Bilateral Tonsillectomy—Cryptic Tonsils
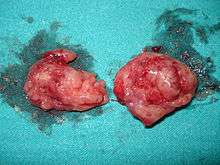 Two removed tonsils.
Two removed tonsils. Throat 1 day after a tonsillectomy.
Throat 1 day after a tonsillectomy. Throat some days after a tonsillectomy.
Throat some days after a tonsillectomy.
See also
References
- 1 2 3 4 5 6 7 McNeill RA (June 1960). "A History of Tonsillectomy: Two Millenia of Trauma, Haemorrhage and Controversy". The Ulster Medical Journal. 29 (1): 59–63. PMC 2384338. PMID 20476427.
- ↑ Paradise JL (1983). "Tonsillectomy and Adenoidectomy" (PDF). II IAPO/IFOS Pediatric ENT Manual. pp. 122–26.
- ↑ "Clinical Indicators Tonsillectomy, Adenoidectomy, Adenotonillectomy, Clinical Indicators Compendium". American Academy of Otolaryngology – Head and Neck Surgery. 2012. Archived from the original on 2 November 2009.
- ↑ Svoboda E (31 August 2009). "In Tonsils, a Problem the Size of a Pea". The New York Times. Retrieved 8 January 2011.
- 1 2 Baugh RF, Archer SM, Mitchell RB, Rosenfeld RM, Amin R, Burns JJ, Darrow DH, Giordano T, Litman RS, Li KK, Mannix ME, Schwartz RH, Setzen G, Wald ER, Wall E, Sandberg G, Patel MM (January 2011). "Clinical practice guideline: tonsillectomy in children". Otolaryngology–Head and Neck Surgery. 144 (1 Suppl): S1–30. doi:10.1177/0194599810389949. PMID 21493257.
- ↑ Randel A (September 2011). "AAO-HNS Guidelines for Tonsillectomy in Children and Adolescents". American Family Physician. 84 (5): 566–73. PMID 21888309.
- ↑ Hornibrook J (July 2009). "The role of tonsillectomy in reducing recurrent pharyngitis: a systematic review". Otolaryngology–Head and Neck Surgery. 141 (1): 155, author reply 155–6. doi:10.1016/j.otohns.2009.04.017. PMID 19559982.
- ↑ Blakley BW, Magit AE (March 2009). "The role of tonsillectomy in reducing recurrent pharyngitis: a systematic review". Otolaryngology–Head and Neck Surgery. 140 (3): 291–7. doi:10.1016/j.otohns.2008.12.013. PMID 19248931.
- 1 2 3 4 5 6 7 8 Burton MJ, Glasziou PP, Chong LY, Venekamp RP (November 2014). "Tonsillectomy or adenotonsillectomy versus non-surgical treatment for chronic/recurrent acute tonsillitis". The Cochrane Database of Systematic Reviews. 11 (11): CD001802. doi:10.1002/14651858.CD001802.pub3. PMID 25407135.
- ↑ van Staaij BK, van den Akker EH, van der Heijden GJ, Schilder AG, Hoes AW (January 2005). "Adenotonsillectomy for upper respiratory infections: evidence based?". Archives of Disease in Childhood. 90 (1): 19–25. doi:10.1136/adc.2003.047530. PMC 1720065. PMID 15613505.
- ↑ Fry J (January 1957). "Are all "T's and A's" really necessary?". British Medical Journal. 1 (5011): 124–9. doi:10.1136/bmj.1.5011.124. PMC 1974118. PMID 13383209.
- ↑ van Staaij BK, van den Akker EH, Rovers MM, Hordijk GJ, Hoes AW, Schilder AG (September 2004). "Effectiveness of adenotonsillectomy in children with mild symptoms of throat infections or adenotonsillar hypertrophy: open, randomised controlled trial". BMJ. 329 (7467): 651. doi:10.1136/bmj.38210.827917.7C. PMC 517640. PMID 15361407.
- ↑ Morad A, Sathe NA, Francis DO, McPheeters ML, Chinnadurai S (February 2017). "Tonsillectomy Versus Watchful Waiting for Recurrent Throat Infection: A Systematic Review". Pediatrics. 139 (2): e20163490. doi:10.1542/peds.2016-3490. PMC 5260157. PMID 28096515.
- 1 2 Marshall T (2002-12-01). "Effectiveness of tonsillectomy? A reply to Howel et al". Family Practice. 19 (6): 707–708. doi:10.1093/fampra/19.6.707-a. ISSN 0263-2136.
- 1 2 3 4 5 Mckee WJ (May 1961). "An interim report on a tonsillectomy survey". Proceedings of the Royal Society of Medicine. 54 (5): 399–402. PMC 1869538. PMID 13774023.
- ↑ Burton MJ, Glasziou PP, Chong LY, Venekamp RP (November 2014). "Tonsillectomy or adenotonsillectomy versus non-surgical treatment for chronic/recurrent acute tonsillitis". The Cochrane Database of Systematic Reviews (11): CD001802. doi:10.1002/14651858.CD001802.pub3. PMID 25407135.
- ↑ Goodman DC, Challener GJ (May 2012). "Tonsillectomy: a procedure in search of evidence". The Journal of Pediatrics. 160 (5): 716–8. doi:10.1016/j.jpeds.2012.01.033. PMID 22336579.
- ↑ Marshall T (June 1998). "A review of tonsillectomy for recurrent throat infection". The British Journal of General Practice. 48 (431): 1331–5. PMC 1410132. PMID 9747553.
- ↑ Paradise JL, Bluestone CD, Colborn DK, Bernard BS, Rockette HE, Kurs-Lasky M (July 2002). "Tonsillectomy and adenotonsillectomy for recurrent throat infection in moderately affected children". Pediatrics. 110 (1 Pt 1): 7–15. doi:10.1542/peds.110.1.7. PMID 12093941.
- 1 2 Venekamp RP, Hearne BJ, Chandrasekharan D, Blackshaw H, Lim J, Schilder AG (October 2015). "Tonsillectomy or adenotonsillectomy versus non-surgical management for obstructive sleep-disordered breathing in children". The Cochrane Database of Systematic Reviews (10): CD011165. doi:10.1002/14651858.CD011165.pub2. PMID 26465274.
- ↑ Clinical trial number NCT02562040 for "Pediatric Adenotonsillectomy for Snoring (PATS)" at ClinicalTrials.gov
- ↑ Clinical trial number NCT02315911 for "Randomized Control Trials of Surgery for Pediatric OSA" at ClinicalTrials.gov
- ↑ McPherson K, Wennberg JE, Hovind OB, Clifford P (November 1982). "Small-area variations in the use of common surgical procedures: an international comparison of New England, England, and Norway". The New England Journal of Medicine. 307 (21): 1310–4. doi:10.1056/NEJM198211183072104. PMID 7133068.
- ↑ Suleman M, Clark MP, Goldacre M, Burton M (April 2010). "Exploring the variation in paediatric tonsillectomy rates between English regions: a 5-year NHS and independent sector data analysis". Clinical Otolaryngology. 35 (2): 111–7. doi:10.1111/j.1749-4486.2010.02086.x. PMID 20500580.
- ↑ "Billions of NHS money wasted on 'ineffective' operations". Evening Standard. Retrieved 2018-01-27.
- ↑ "Dr. Obama's Tonsillectomy". Wall Street Journal. 2009-07-27. ISSN 0099-9660. Retrieved 2017-10-18.
- ↑ Bolande RP (March 1969). "Ritualistic surgery--circumcision and tonsillectomy". The New England Journal of Medicine. 280 (11): 591–6. doi:10.1056/NEJM196903132801105. PMID 4885060.
- ↑ Furman RA (February 1959). "Handling parental pressure for T and A". The Journal of Pediatrics. 54 (2): 195–9. doi:10.1016/S0022-3476(59)80062-7. PMID 13621366.
- ↑ Burton MJ (February 2008). "Commentary: Tonsillectomy--then and now". International Journal of Epidemiology. 37 (1): 23–5. doi:10.1093/ije/dym259. PMID 18184674.
- ↑ Berger R (September 1976). "The question of tonsillectomy and adenoidectomy: still with us in 1976". The Journal of the American Osteopathic Association. 76 (1): 32–4. PMID 1048964.
- ↑ Marshall T (June 1999). "How many tonsillectomies are based on evidence from randomized controlled trials?". The British Journal of General Practice : The Journal of the Royal College of General Practitioners. 49 (443): 487–8. PMC 1313456. PMID 10562758.
- ↑ Walton J, Ebner Y, Stewart MG, April MM (March 2012). "Systematic review of randomized controlled trials comparing intracapsular tonsillectomy with total tonsillectomy in a pediatric population". Archives of Otolaryngology--Head & Neck Surgery. 138 (3): 243–9. doi:10.1001/archoto.2012.16. PMID 22431869.
- ↑ "COBLATION Plasma Technology - ENT". Smith & Nephew US Professional. Retrieved 15 July 2016.
- ↑ Friedman M, LoSavio P, Ibrahim H, Ramakrishnan V (May 2003). "Radiofrequency tonsil reduction: safety, morbidity, and efficacy". The Laryngoscope. 113 (5): 882–7. doi:10.1097/00005537-200305000-00020. PMID 12792327.
- ↑ Windfuhr JP (May 2007). "[Coblation tonsillectomy: a review of the literature]". Hno. 55 (5): 337–48. doi:10.1007/s00106-006-1523-3. PMID 17431570.
- ↑ Hong SM, Cho JG, Chae SW, Lee HM, Woo JS (June 2013). "Coblation vs. Electrocautery Tonsillectomy: A Prospective Randomized Study Comparing Clinical Outcomes in Adolescents and Adults". Clinical and Experimental Otorhinolaryngology. 6 (2): 90–3. doi:10.3342/ceo.2013.6.2.90. PMC 3687068. PMID 23799166.
- ↑ Omrani M, Barati B, Omidifar N, Okhovvat AR, Hashemi SA (January 2012). "Coblation versus traditional tonsillectomy: A double blind randomized controlled trial". Journal of Research in Medical Sciences. 17 (1): 45–50. PMC 3523437. PMID 23248656.
- ↑ Walner DL, Miller SP, Villines D, Bussell GS (October 2012). "Coblation tonsillectomy in children: incidence of bleeding". The Laryngoscope. 122 (10): 2330–6. doi:10.1002/lary.23526. PMID 22833366.
- ↑ Khan I, Abelardo E, Scott NW, Shakeel M, Menakaya O, Jaramillo M, Mahmood K (February 2012). "Coblation tonsillectomy: is it inherently bloody?". European Archives of Oto-Rhino-Laryngology. 269 (2): 579–83. doi:10.1007/s00405-011-1609-8. PMID 21547390.
- ↑ Mösges R, Hellmich M, Allekotte S, Albrecht K, Böhm M (June 2011). "Hemorrhage rate after coblation tonsillectomy: a meta-analysis of published trials". European Archives of Oto-Rhino-Laryngology. 268 (6): 807–16. doi:10.1007/s00405-011-1535-9. PMC 3087106. PMID 21373898.
- ↑ Beloso, A (November 2003). "Coblation tonsillectomy versus dissection tonsillectomy: postoperative hemorrhage". The Laryngoscope. 113 (11): 2010–2013. doi:10.1097/00005537-200311000-00029.
- ↑ "COBLATION Tonsillectomy - My Tonsils". My Tonsils.com. Retrieved 11 July 2016.
- ↑ "Interventional procedure overview of laser assisted serial tonsillectomy" (PDF). National institute of clinical excellence. Retrieved 30 November 2013.
- ↑ Graham JM, Scadding GK, Bull PD (2008). Pediatric ENT. Springer. p. 136. ISBN 978-3-540-69930-9.
- ↑ Timby BK, Nancy Ellen Smith (2006). Introductory medical-surgical nursing. Lippincott Williams & Wilkins. p. 357. ISBN 978-0-7817-8032-2.
- ↑ Pemberton CM (1988). Mayo Clinic diet manual. B.C. Decker. ISBN 978-1-55664-032-2.
- ↑ Windfuhr JP, Chen YS, Remmert S (February 2005). "Hemorrhage following tonsillectomy and adenoidectomy in 15,218 patients". Otolaryngology–Head and Neck Surgery. 132 (2): 281–6. doi:10.1016/j.otohns.2004.09.007. PMID 15692542.
- ↑ Møiniche S, Rømsing J, Dahl JB, Tramèr MR (January 2003). "Nonsteroidal antiinflammatory drugs and the risk of operative site bleeding after tonsillectomy: a quantitative systematic review". Anesthesia and Analgesia. 96 (1): 68–77, table of contents. doi:10.1213/00000539-200301000-00015. PMID 12505926.
- ↑ Chimona T, Proimos E, Mamoulakis C, Tzanakakis M, Skoulakis CE, Papadakis CE (September 2008). "Multiparametric comparison of cold knife tonsillectomy, radiofrequency excision and thermal welding tonsillectomy in children". International Journal of Pediatric Otorhinolaryngology. 72 (9): 1431–6. doi:10.1016/j.ijporl.2008.06.006. PMID 18620759.
- ↑ Graumüller S, Laudien B (November 2003). Postoperative pain after tonsillectomy—comparison of children and adults. Advances in Pediatric ORL. Proceedings of the 8th International Congress of Pediatric Otorhinolaryngology. 1254. Elsevier. pp. 469–72. doi:10.1016/S0531-5131(03)01073-2.
- ↑ Coté CJ, Posner KL, Domino KB (June 2014). "Death or neurologic injury after tonsillectomy in children with a focus on obstructive sleep apnea: houston, we have a problem!". Anesthesia and Analgesia. 118 (6): 1276–83. doi:10.1213/ANE.0b013e318294fc47. PMID 23842193.
- ↑ Randall DA, Hoffer ME (January 1998). "Complications of tonsillectomy and adenoidectomy". Otolaryngology–Head and Neck Surgery. 118 (1): 61–8. doi:10.1016/S0194-5998(98)70376-6. PMID 9450830.
- ↑ Ilk HG, Eroğul O, Satar B, Ozkaptan Y (December 2002). "Effects of tonsillectomy on speech spectrum". Journal of Voice : Official Journal of the Voice Foundation. 16 (4): 580–6. doi:10.1016/S0892-1997(02)00133-9. PMID 12512645.
- ↑ Tomofuji S, Sakagami M, Kushida K, Terada T, Mori H, Kakibuchi M (December 2005). "Taste disturbance after tonsillectomy and laryngomicrosurgery". Auris, Nasus, Larynx. 32 (4): 381–6. doi:10.1016/j.anl.2005.05.005. PMID 16046093.
- ↑ Tomita H, Ohtuka K (2002). "Taste disturbance after tonsillectomy". Acta Oto-laryngologica. Supplementum. 122 (546): 164–72. doi:10.1080/00016480260046571. PMID 12132617.
- ↑ Backeljauw B, Holland SK, Altaye M, Loepke AW (July 2015). "Cognition and Brain Structure Following Early Childhood Surgery With Anesthesia". Pediatrics. 136 (1): e1–12. doi:10.1542/peds.2014-3526. PMC 4485006. PMID 26055844.
- ↑ Mesa Suárez P, Santotoribio JD, Ramos Ramos V, González García MÁ, Pérez Ramos S, Portilla Huertas D, Muñoz Hoyos A (May 2016). "[Brain damage after general anesthesia]". Medicina Clinica. 146 (9): 384–8. doi:10.1016/j.medcli.2016.01.018. PMID 26969427.
- ↑ Ing C, DiMaggio C, Whitehouse A, Hegarty MK, Brady J, von Ungern-Sternberg BS, Davidson A, Wood AJ, Li G, Sun LS (September 2012). "Long-term differences in language and cognitive function after childhood exposure to anesthesia". Pediatrics. 130 (3): e476–85. doi:10.1542/peds.2011-3822. PMID 22908104.
- ↑ Johnson RF, Chang A, Mitchell RB (April 2018). "Nationwide readmissions after tonsillectomy among pediatric patients - United States". International Journal of Pediatric Otorhinolaryngology. 107: 10–13. doi:10.1016/j.ijporl.2018.01.026. PMID 29501287.
- ↑ Lee KL (2008). Essential Otolaryngology: Head and Neck Surgery, Ninth Edition. McGraw-Hill Professional. p. 544. ISBN 978-0-07-148270-7.
- 1 2 3 Steward DL, Grisel J, Meinzen-Derr J (August 2011). Steward DL, ed. "Steroids for improving recovery following tonsillectomy in children". The Cochrane Database of Systematic Reviews (8): CD003997. doi:10.1002/14651858.CD003997.pub2. PMID 21833946.
- ↑ Wijga AH, Scholtens S, Wieringa MH, Kerkhof M, Gerritsen J, Brunekreef B, Smit HA (April 2009). "Adenotonsillectomy and the development of overweight". Pediatrics. 123 (4): 1095–101. doi:10.1542/peds.2008-1502. PMID 19336367.
- ↑ Wei JL (June 2011). "Weight gain after tonsillectomy: myth or reality? Interpreting research responsibly". Otolaryngology–Head and Neck Surgery. 144 (6): 855–7. doi:10.1177/0194599811406674. PMID 21515804.
- ↑ Liaw KL, Adami J, Gridley G, Nyren O, Linet MS (September 1997). "Risk of Hodgkin's disease subsequent to tonsillectomy: a population-based cohort study in Sweden". International Journal of Cancer. 72 (5): 711–3. doi:10.1002/(sici)1097-0215(19970904)72:5<711::aid-ijc1>3.0.co;2-v. PMID 9311582.
- ↑ Vianna NJ, Greenwald P, Davies JN (February 1971). "Tonsillectomy and Hodgkin's disease: the lymphoid tissue barrier". Lancet. 1 (7696): 431–2. doi:10.1016/s0140-6736(71)92416-0. PMID 4100403.
- ↑ Vianna NJ, Lawrence CE, Davies JN, Arbuckle J, Harris S, Marani W, Wilkinson J (August 1980). "Tonsillectomy and childhood Hodgkin's disease". Lancet. 2 (8190): 338–40. doi:10.1016/S0140-6736(80)90339-6. PMID 6105477.
- ↑ Kirchhoff LV, Evans AS, McClelland KE, Carvalho RP, Pannuti CS (November 1980). "A case-control study of Hodgkin's disease in Brazil. I. Epidemiogic aspects". American Journal of Epidemiology. 112 (5): 595–608. doi:10.1093/oxfordjournals.aje.a113032. PMID 7435488.
- ↑ Wang J, Mack TM, Hwang A, Nathwani BN, Hamilton A, Cozen W (2011-11-18). "Innmune-Related Risk Factors for Non-Hodgkin Lymphoma in Twins". Blood. 118 (21): 1588. ISSN 0006-4971.
- ↑ Sokic SI, Adanja BJ, Marinkovic JP, Vlajinac HD (August 1995). "Risk factors for laryngeal cancer". European Journal of Epidemiology. 11 (4): 431–3. doi:10.1007/BF01721228. PMID 8549710.
- ↑ Garman KS, Boutte HJ, Furstenberg RJ, Chiu S, Lloyd B, Zhang C, Onaitis M, Chow S, McCall SJ (2016). "Tu1179 Previous Tonsillectomy Is Associated With Increased Risk of Esophageal Cancer". Gastroenterology. 150 (4): S856. doi:10.1016/s0016-5085(16)32889-x.
- ↑ Bross ID (1971-11-01). "Some Epidemiological Clues in Thyroid Cancer". Archives of Internal Medicine. 128 (5): 755–60. doi:10.1001/archinte.1971.00310230085006. PMID 4256163.
- 1 2 Raso AM, Dorigo M, Terrando R (November 1975). "[Statistical analysis of correlations between tonsillectomy and malignant neoplasms of the thyroid]". Minerva Chirurgica. 30 (22): 1135–9. PMID 1228489.
- ↑ Lubin JH, Burns PE, Blot WJ, Lees AW, May C, Morris LE, Fraumeni JF (February 1982). "Risk factors for breast cancer in women in northern Alberta, Canada, as related to age at diagnosis". Journal of the National Cancer Institute. 68 (2): 211–7. doi:10.1093/jnci/68.2.211. PMID 6950154.
- ↑ Brasky TM, Bonner MR, Dorn J, Marhsall JR, Vena JE, Brasure JR, Freudenheim JL (April 2009). "Tonsillectomy and breast cancer risk in the Western New York Diet Study". Cancer Causes & Control. 20 (3): 369–74. doi:10.1007/s10552-008-9251-5. PMID 18953693.
- 1 2 Sun LM, Chen HJ, Li TC, Sung FC, Kao CH (January 2015). "A nationwide population-based cohort study on tonsillectomy and subsequent cancer incidence". The Laryngoscope. 125 (1): 134–9. doi:10.1002/lary.24864. PMID 25130597.
- ↑ Whittemore AS, Paffenbarger RS, Anderson K, Lee JE (December 1984). "Early precursors of urogenital cancers in former college men". The Journal of Urology. 132 (6): 1256–61. doi:10.1016/s0022-5347(17)50118-4. PMID 6502830.
- ↑ Zevallos JP, Mazul AL, Rodriguez N, Weissler MC, Brennan P, Anantharaman D, Abedi-Ardekani B, Neil Hayes D, Olshan AF (March 2016). "Previous tonsillectomy modifies odds of tonsil and base of tongue cancer". British Journal of Cancer. 114 (7): 832–8. doi:10.1038/bjc.2016.63. PMC 4984870. PMID 26977858.
- ↑ Paffenbarger RS, Wing AL, Hyde RT (January 1978). "Characteristics in youth predictive of adult-onset malignant lymphomas, melanomas, and leukemias: brief communication". Journal of the National Cancer Institute. 60 (1): 89–92. doi:10.1093/jnci/60.1.89. PMID 272469.
- ↑ Schüz J, Kaletsch U, Meinert R, Kaatsch P, Michaelis J (May 1999). "Association of childhood leukaemia with factors related to the immune system". British Journal of Cancer. 80 (3–4): 585–90. doi:10.1038/sj.bjc.6690395. PMC 2362320. PMID 10408870.
- ↑ Cuneo JM (April 1972). "Tonsillectomy and leukaemia". Lancet. 1 (7755): 846–7. doi:10.1016/s0140-6736(72)90829-x. PMID 4111604.
- ↑ "Investigating pediatric cancer risk utilizing the Utah population database - ProQuest". search.proquest.com. Retrieved 2018-03-05.
- ↑ Anderson HR, Bland JM, Peckham CS (June 1987). "Risk factors for asthma up to 16 years of age. Evidence from a national cohort study". Chest. 91 (6 Suppl): 127S–130S. doi:10.1378/chest.91.6_supplement.127s. PMID 3581954.
- 1 2 3 4 5 6 7 8 9 10 11 Byars SG, Stearns SC, Boomsma JJ (July 2018). "Association of Long-Term Risk of Respiratory, Allergic, and Infectious Diseases With Removal of Adenoids and Tonsils in Childhood". JAMA Otolaryngology–Head & Neck Surgery. 144 (7): 594–603. doi:10.1001/jamaoto.2018.0614. PMID 29879264.
- ↑ Sultész M, Katona G, Hirschberg A, Gálffy G (May 2010). "Prevalence and risk factors for allergic rhinitis in primary schoolchildren in Budapest". International Journal of Pediatric Otorhinolaryngology. 74 (5): 503–9. doi:10.1016/j.ijporl.2010.02.008. PMID 20211496.
- ↑ Matheson MC, Walters EH, Simpson JA, Wharton CL, Ponsonby AL, Johns DP, Jenkins MA, Giles GG, Hopper JL, Abramson MJ, Dharmage SC (March 2009). "Relevance of the hygiene hypothesis to early vs. late onset allergic rhinitis". Clinical and Experimental Allergy. 39 (3): 370–8. doi:10.1111/j.1365-2222.2008.03175.x. PMID 19187325.
- ↑ Basseri RJ, Chong K, Chang C, Pimentel M (2011). "History of tonsillectomy is associated with irritable bowel syndrome". Journal of Clinical Gastroenterology. 45 (10): 912. doi:10.1097/MCG.0b013e31822a289f. PMID 21857532.
- ↑ Sun W, Han X, Wu S, Yang C (June 2016). "Tonsillectomy and the risk of inflammatory bowel disease: A systematic review and meta-analysis". Journal of Gastroenterology and Hepatology. 31 (6): 1085–94. doi:10.1111/jgh.13273. PMID 26678358.
- ↑ Koutroubakis IE, Vlachonikolis IG, Kapsoritakis A, Spanoudakis S, Roussomoustakaki M, Mouzas IA, Kouroumalis EA, Manousos ON (February 1999). "Appendectomy, tonsillectomy, and risk of inflammatory bowel disease: case-controlled study in Crete". Diseases of the Colon and Rectum. 42 (2): 225–30. doi:10.1007/BF02237133. PMID 10211500.
- ↑ Gearry RB, Richardson AK, Frampton CM, Dodgshun AJ, Barclay ML (February 2010). "Population-based cases control study of inflammatory bowel disease risk factors". Journal of Gastroenterology and Hepatology. 25 (2): 325–33. doi:10.1111/j.1440-1746.2009.06140.x. PMID 20074146.
- ↑ Wurzelmann JI, Lyles CM, Sandler RS (March 1994). "Childhood infections and the risk of inflammatory bowel disease". Digestive Diseases and Sciences. 39 (3): 555–60. doi:10.1007/BF02088342. PMID 8131692.
- ↑ Spehlmann ME, Begun AZ, Saroglou E, Hinrichs F, Tiemann U, Raedler A, Schreiber S (February 2012). "Risk factors in German twins with inflammatory bowel disease: results of a questionnaire-based survey". Journal of Crohn's & Colitis. 6 (1): 29–42. doi:10.1016/j.crohns.2011.06.007. PMID 22261525.
- ↑ Andreu Ballester JC, Ballester F, Colomer Rubio E, Millán Scheiding M (March 2005). "Association between tonsillectomy, adenoidectomy, and appendicitis". Revista Espanola de Enfermedades Digestivas : Organo Oficial de la Sociedad Espanola de Patologia Digestiva. 97 (3): 179–86. doi:10.4321/s1130-01082005000300006. PMID 15839812.
- ↑ Binning G (November 1950). "The influence of the perturbations of childhood life upon the occurrence of appendectomy". Canadian Medical Association Journal. 63 (5): 461–7. PMC 1821799. PMID 14778094.
- ↑ Janszky I, Mukamal KJ, Dalman C, Hammar N, Ahnve S (September 2011). "Childhood appendectomy, tonsillectomy, and risk for premature acute myocardial infarction--a nationwide population-based cohort study". European Heart Journal. 32 (18): 2290–6. doi:10.1093/eurheartj/ehr137. PMID 21632600.
- ↑ Sawahata M, Nakamura Y, Sugiyama Y (May 2017). "Appendectomy, tonsillectomy, and risk for sarcoidosis - A hospital-based case-control study in Japan". Respiratory Investigation. 55 (3): 196–202. doi:10.1016/j.resinv.2016.12.004. PMID 28427746.
- ↑ Fernandez-Madrid F, Reed AH, Karvonen RL, Granda JL (February 1985). "Influence of antecedent lymphoid surgery on the odds of acquiring rheumatoid arthritis". The Journal of Rheumatology. 12 (1): 43–8. PMID 3981518.
- ↑ Gottlieb NL, Page WF, Appelrouth DJ, Palmer R, Kiem IM (1979). "Antecedent tonsillectomy and appendectomy in rheumatoid arthritis". The Journal of Rheumatology. 6 (3): 316–23. PMID 490526.
- ↑ Duval M, Daniel SJ (December 2008). "Retropharyngeal and parapharyngeal abscesses or phlegmons in children. Is there an association with adenotonsillectomy?". International Journal of Pediatric Otorhinolaryngology. 72 (12): 1765–9. doi:10.1016/j.ijporl.2008.07.007. PMID 18922587.
- ↑ Marchisio P, Principi N, Passali D, Salpietro DC, Boschi G, Chetrì G, Caramia G, Longhi R, Reali E, Meloni G, De Santis A, Sacher B, Cupido G (July 1998). "Epidemiology and treatment of otitis media with effusion in children in the first year of primary school". Acta Oto-Laryngologica. 118 (4): 557–62. doi:10.1080/00016489850154720. PMID 9726683.
- ↑ Poskanzer DC (December 1965). "Tonsillectomy and multiple sclerosis". Lancet. 2 (7425): 1264–6. doi:10.1016/S0140-6736(65)92281-6. PMID 4165404.
- ↑ Lamoureux G, Giard N, Jolicoeur R, Toughlian V, Desrosiers M (January 1976). "Immunological features in multiple sclerosis". British Medical Journal. 1 (6003): 183–6. doi:10.1136/bmj.1.6003.183. PMC 1638425. PMID 764920.
- ↑ Grønning M, Riise T, Kvåle G, Albrektsen G, Midgard R, Nyland H (1993). "Infections in childhood and adolescence in multiple sclerosis. A case-control study". Neuroepidemiology. 12 (2): 61–9. doi:10.1159/000110302. PMID 8232705.
- ↑ Lunny C, Knopp-Sihota JA, Fraser SN (May 2013). "Surgery and risk for multiple sclerosis: a systematic review and meta-analysis of case-control studies". BMC Neurology. 13: 41. doi:10.1186/1471-2377-13-41. PMC 3651719. PMID 23648120.
- ↑ Wang YP, Wang MC, Lin HC, Lee KS, Chou P (2015-04-07). "Tonsillectomy and the risk for deep neck infection-a nationwide cohort study". PLOS One. 10 (4): e0117535. doi:10.1371/journal.pone.0117535. PMC 4388732. PMID 25849535.
- ↑ Ogra PL (January 1971). "Effect of tonsillectomy and adenoidectomy on nasopharyngeal antibody response to poliovirus". The New England Journal of Medicine. 284 (2): 59–64. doi:10.1056/NEJM197101142840201. PMID 4321186.
- ↑ Francis T, Krill CE, Toomey JA, Mack WN (1942-08-22). "Poliomyelitis Following Tonsillectomy in Five Members of a Family: An Epidemiologic Study". JAMA: The Journal of the American Medical Association. 119 (17): 1392–1396. doi:10.1001/jama.1942.02830340004002.
- ↑ Anderson JA (1945). "Poliomyelitis and recent tonsillectomy". The Journal of Pediatrics. 27 (1): 68–70. doi:10.1016/s0022-3476(45)80208-1.
- ↑ Barsky P, Lauer R (September 1957). "Tonsillectomy and the risk of poliomyelitis". Canadian Medical Association Journal. 77 (6): 576–8. PMC 1824413. PMID 13460884.
- ↑ Karppelin M, Siljander T, Huhtala H, Aromaa A, Vuopio J, Hannula-Jouppi K, Kere J, Syrjänen J (March 2013). "Recurrent cellulitis with benzathine penicillin prophylaxis is associated with diabetes and psoriasis". European Journal of Clinical Microbiology & Infectious Diseases. 32 (3): 369–72. doi:10.1007/s10096-012-1751-2. PMID 23007460.
- ↑ Parikh-Patel A, Gold EB, Worman H, Krivy KE, Gershwin ME (January 2001). "Risk factors for primary biliary cirrhosis in a cohort of patients from the united states". Hepatology. 33 (1): 16–21. doi:10.1053/jhep.2001.21165. PMID 11124815.
- ↑ Gershwin ME, Selmi C, Worman HJ, Gold EB, Watnik M, Utts J, Lindor KD, Kaplan MM, Vierling JM (November 2005). "Risk factors and comorbidities in primary biliary cirrhosis: a controlled interview-based study of 1032 patients". Hepatology. 42 (5): 1194–202. doi:10.1002/hep.20907. PMC 3150736. PMID 16250040.
- ↑ Chung SD, Lin HC, Wu CS, Kao LT, Hung SH (December 2016). "A tonsillectomy increased the risk of chronic rhinosinusitis among children: A three-year follow-up study". International Journal of Pediatric Otorhinolaryngology. 91: 82–85. doi:10.1016/j.ijporl.2016.09.038. PMID 27863647.
- ↑ Pino Rivero V, Marcos García M, Trinidad Ruiz G, Pardo Romero G, González Palomino A, Keituqwa Yáñez T, Rejas Ugena E, Blasco Huelva A (2004). "[Lingual tonsillitis. Report of 3 cases and literature review]". Anales Otorrinolaringologicos Ibero-Americanos. 31 (6): 557–63. PMID 15663087.
- ↑ Guttman D, Jacob S (December 2014). "Lingual tonsil hypertrophy in patients with a history of palatine tonsillectomy" (PDF). Medical Connections. 9 (4): 43–46.
- ↑ Murphy TK, Storch EA, Lewin AB, Edge PJ, Goodman WK (February 2012). "Clinical factors associated with pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections". The Journal of Pediatrics. 160 (2): 314–9. doi:10.1016/j.jpeds.2011.07.012. PMC 3227761. PMID 21868033.
- 1 2 Cantani A, Bellioni P, Salvinelli F, Businco L (December 1986). "Serum immunoglobulins and secretory IgA deficiency in tonsillectomized children". Annals of Allergy. 57 (6): 413–6. PMID 3789468.
- ↑ Andreu-Ballester JC, Pérez-Griera J, Ballester F, Colomer-Rubio E, Ortiz-Tarín I, Peñarroja Otero C (June 2007). "Secretory immunoglobulin A (sIgA) deficiency in serum of patients with GALTectomy (appendectomy and tonsillectomy)". Clinical Immunology. 123 (3): 289–97. doi:10.1016/j.clim.2007.02.004. PMID 17449327.
- ↑ Brandtzaeg P (1996-01-01). "The B-cell development in tonsillar lymphoid follicles". Acta Oto-Laryngologica. Supplementum. 523: 55–9. PMID 9082810.
- ↑ Kim J, Morris M. "Long-Term Effects of Tonsillectomy on Immunity" (PDF). Georgetown University School of Medicine, Washington, D.C.
- ↑ Ji J, Sundquist J, Sundquist K (August 2016). "Tonsillectomy associated with an increased risk of autoimmune diseases: A national cohort study". Journal of Autoimmunity. 72: 1–7. doi:10.1016/j.jaut.2016.06.007. PMID 27344241.
- ↑ Mészáros D, Dharmage SC, Matheson MC, Venn A, Wharton CL, Johns DP, Abramson MJ, Giles GG, Hopper JL, Walters EH (June 2010). "Poor lung function and tonsillectomy in childhood are associated with mortality from age 18 to 44". Respiratory Medicine. 104 (6): 808–15. doi:10.1016/j.rmed.2009.12.001. PMID 20079616.
- ↑ Johansson E, Hultcrantz E (September 2003). "Tonsillectomy--clinical consequences twenty years after surgery?". International Journal of Pediatric Otorhinolaryngology. 67 (9): 981–8. doi:10.1016/S0165-5876(03)00196-4. PMID 12907054.
Further reading
- Kramer SP, Pasha R (2005). Otolaryngology: Head and Neck Surgery--A Clinical & Reference Guide, Second Edition. Plural Publishing. ISBN 978-1-59756-023-8.
- Montgomery WR (1996). Surgery of the Upper Respiratory System. Baltimore: Williams & Wilkins. ISBN 978-0-683-06121-5.
- Nsow JB, Wackym PA (2009). Ballenger's Otorhinolaryngology Head and Neck Surgery, 17th edition (Otorhinolaryngology: Head and Neck Surgery (Ballenger)). pmph usa. ISBN 978-1-55009-337-7.
- "Clinical UM Guideline CG-SURG-30: Tonsillectomy for Children". Blue Cross Blue Shield Association of Georgia.
External links
| Wikimedia Commons has media related to Tonsillectomy. |
- Tonsillectomy Procedures
- ENT Matters: Tonsillectomy
- drtbalu otolaryngology on line
- History of tonsillectomy
- Tonsillectomy new vistas
- Laser Tonsillectomy Procedure
- Study: Tonsil and adenoid removal associated with respiratory diseases, allergies and infections
- Having tonsils out as a child increases risk of infections and lung complaints for life, finds study