Peripheral artery disease
| Peripheral artery disease | |
|---|---|
| Synonyms | Peripheral vascular disease (PVD), peripheral artery occlusive disease, peripheral obliterative arteriopathy |
 | |
| An arterial insufficiency ulcer in a person with severe peripheral artery disease | |
| Specialty | Vascular surgery |
| Symptoms | Leg pain when walking which resolves with rest, skin ulcers, bluish skin, cold skin[1][2] |
| Complications | Infection, amputation[3] |
| Causes | Atherosclerosis, artery spasm[4][5] |
| Risk factors | Cigarette smoking, diabetes, high blood pressure, high blood cholesterol.[3][6] |
| Diagnostic method | Ankle-brachial index < 0.90, duplex ultrasonography, angiography[7][8] |
| Treatment | Stopping smoking, supervised exercise therapy, surgery[9][10][11] |
| Medication | Statins, ACE inhibitors, cilostazol[11] |
| Frequency | 155 million (2015)[12] |
| Deaths | 52,500 (2015)[13] |
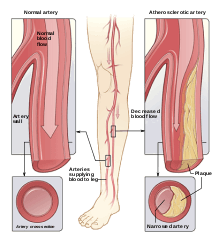
Peripheral artery disease (PAD) is a narrowing of the arteries other than those that supply the heart or the brain.[4] When narrowing occurs in the heart, it is called coronary artery disease, while, in the brain, it is called cerebrovascular disease. Peripheral artery disease most commonly affects the legs, but other arteries may also be involved.[3] The classic symptom is leg pain when walking which resolves with rest, known as intermittent claudication.[1] Other symptoms including skin ulcers, bluish skin, cold skin, or poor nail and hair growth may occur in the affected leg.[2] Complications may include an infection or tissue death which may require amputation; coronary artery disease, or stroke.[3] Up to 50% of cases of PAD are without symptoms.[1]
The main risk factor is cigarette smoking.[3] Other risk factors include diabetes, high blood pressure, and high blood cholesterol.[6] The underlying mechanism is usually atherosclerosis.[5] Other causes include artery spasm.[4] PAD is typically diagnosed by finding an ankle-brachial index (ABI) less than 0.90, which is the systolic blood pressure at the ankle divided by the systolic blood pressure of the arm.[8] Duplex ultrasonography and angiography may also be used.[7] Angiography is more accurate and allows for treatment at the same time; however, it is associated with greater risks.[8]
It is unclear if screening for disease is useful as it has not been properly studied.[14][15] In those with intermittent claudication from PAD, stopping smoking and supervised exercise therapy improves outcomes.[10][11] Medications, including statins, ACE inhibitors, and cilostazol also may help.[11][16] Aspirin does not appear to help those with mild disease but is usually recommended in those with more significant disease.[17][18] Anticoagulants such as warfarin are not typically of benefit.[19] Procedures used to treat the disease include bypass grafting, angioplasty, and atherectomy.[9]
In 2015 about 155 million people had PAD worldwide.[12] In the developed world it affects about 5.3% of 45 to 50 years olds and 18.6% of 85- to 90-year-olds.[6] In the developing world it affects 4.6% of people between the ages of 45 to 50 and 15% of people between the ages of 85 to 90.[6] In the developed world PAD is equally common among men and women while in the developing world women are more commonly affected.[6] In 2015 PAD resulted in about 52,500 deaths up from 16,000 deaths in 1990.[13][20]
Signs and symptoms

Up to 50% of people with PAD may have no symptoms.[1] Symptoms of PAD in the legs and feet are generally divided into 2 categories:
- Intermittent claudication—pain in muscles when walking or using the affected muscles that is relieved by resting those muscles. This is due to the unmet oxygen demand in muscles with use in the setting of inadequate blood flow.
- Critical limb ischemia, consisting of:
- Rest pain, a pain in the soles of the feet, particularly when the feet are elevated, such as when in bed.
- Tissue loss, consisting of arterial insufficiency ulcers, which are sores or wounds that heal slowly or not at all, and gangrene.
Medical signs of PAD in the legs, due to inadequate perfusion, include:
- Noticeable change in color – blueness, or in temperature (coolness) when compared to the other limb.
- Buerger's test can check for pallor on elevation of limb and redness (rubor) on a change to a sitting position, in an assessment of arterial sufficiency.
- Diminished hair and nail growth on affected limb and digits
PAD in other parts of the body depends on the organ affected. Renal artery stenosis can cause renovascular hypertension. Carotid artery disease can cause strokes and transient ischemic attacks.
Causes
Risk factors contributing to PAD are the same as those for atherosclerosis:[21][22]
- Smoking – tobacco use in any form is the single most important modifiable cause of PAD internationally. Smokers have up to a tenfold increase in relative risk for PAD in a dose-response relationship.[22] Exposure to second-hand smoke from environmental exposure has also been shown to promote changes in blood vessel lining (endothelium) which is a precursor to atherosclerosis. Smokers are 2 to 3 times more likely to have lower extremity peripheral arterial disease than coronary artery disease.[23] More than 80%-90% of patients with lower extremity peripheral arterial disease are current or former smokers.[24] The risk of PAD increases with the number of cigarettes smoked per day and the number of years smoked.[25][26]
- Diabetes mellitus – causes between two and four times increased risk of PAD by causing endothelial and smooth muscle cell dysfunction in peripheral arteries.[27][28][29] The risk of developing lower extremity peripheral arterial disease is proportional to the severity and duration of diabetes.[30]
- Dyslipidemia – a high level of low-density lipoprotein (LDL cholesterol) and a low level of high-density lipoprotein (HDL cholesterol) in the blood) - elevation of total cholesterol, LDL cholesterol, and triglyceride levels each have been correlated with accelerated PAD. Correction of dyslipidemia by diet and/or medication is associated with a major improvement in rates of heart attack and stroke.[31]
- Hypertension – elevated blood pressure is correlated with an increase in the risk of developing PAD, as well as in associated coronary and cerebrovascular events (heart attack and stroke). Hypertension increased the risk of intermittent claudication 2.5- to 4-fold in men and women, respectively.[32]
- Risk of PAD also increases in individuals who are over the age of 50, male, obese, heart attack, or stroke[33][34] or with a family history of vascular disease.[35][36]
- Other risk factors which are being studied include levels of various inflammatory mediators such as C-reactive protein, fibrinogen,[37] hyperviscosity, hypercoagulable state.
Risk factors
Peripheral arterial disease is more common in the following populations of people:[26][38]
- All people who have leg symptoms with exertion (suggestive of claudication) or ischemic rest pain.
- All people aged 65 years and over regardless of risk factor status.
- All people between the age of 50 to 69 and who have a cardiovascular risk factor (particularly diabetes or smoking).
- Age less than 50 years, with diabetes and one other atherosclerosis risk factor (smoking, dyslipidemia, hypertension, or hyperhomocysteinemia).
- Individuals with an abnormal lower extremity pulse examination.
- Those with known atherosclerotic coronary, carotid, or renal artery disease.
- All people with a Framingham risk score 10%-20%
- All people who have previously experienced chest pain
Diagnosis
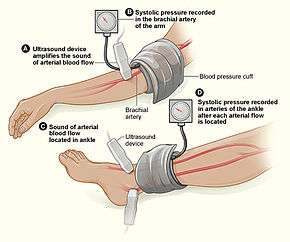
Upon suspicion of PAD, the first-line study is the ankle–brachial index (ABI), which is the ratio of blood pressure in the ankle to blood pressure in the upper arm. When the blood pressure readings in the ankles is lower than that in the arms, blockages in the arteries which provide blood from the heart to the ankle are suspected. An ABI range of 1.00 to 1.40 is considered normal. A person is diagnosed with PAD when the ABI is ≤ 0.90. ABI values of 0.91 to 0.99 are considered borderline and values >1.40 indicate noncompressible arteries. PAD is graded as mild to moderate if the ABI is between 0.41 and 0.90, and an ABI less than 0.40 is suggestive of severe PAD. These relative categories have prognostic value.[26]
In people with suspected PAD but normal resting ABIs, exercise testing of ABI can be done. A base line ABI is obtained prior to exercise. The patient is then asked to exercise (usually patients are made to walk on a treadmill at a constant speed) until claudication pain occurs (or a maximum of 5 minutes), following which the ankle pressure is again measured. A decrease in ABI of 15%-20% would be diagnostic of PAD.[26][38]
It is possible for conditions which stiffen the vessel walls (such as calcifications that occur in the setting of long term diabetes) to produce false negatives usually, but not always, indicated by abnormally high ABIs (> 1.40). Such results and suspicions merit further investigation and higher level studies.[39]
If ABIs are abnormal the next step is generally a lower limb doppler ultrasound examination to look at the site and extent of atherosclerosis. Other imaging can be performed by angiography,[21] where a catheter is inserted into the common femoral artery and selectively guided to the artery in question. While injecting a radiodense contrast agent an X-ray is taken. Any flow limiting stenoses found in the x-ray can be identified and treated by atherectomy, angioplasty or stenting. Contrast angiography is the most readily available and widely used imaging technique.
Modern multislice computerized tomography (CT) scanners provide direct imaging of the arterial system as an alternative to angiography.
Magnetic resonance angiography (MRA) is a noninvasive diagnostic procedure that uses a combination of a large magnet, radio frequencies, and a computer to produce detailed images to provide pictures of blood vessels inside the body. The advantages of MRA include its safety and ability to provide high-resolution three-dimensional (3D) imaging of the entire abdomen, pelvis and lower extremities in one sitting.[40][41]
Classification
Peripheral artery occlusive disease is commonly divided in the Fontaine stages, introduced by René Fontaine in 1954 for chronic limb ischemia:[38][42]
- Stage I: Asymptomatic, incomplete blood vessel obstruction
- Stage II: Mild claudication pain in limb
- Stage IIA: Claudication when walking a distance of greater than 200 meters
- Stage IIB: Claudication when walking a distance of less than 200 meters
A classification by the Society for Vascular Surgery and International Society of Cardiovascular Surgery (SVS/ISCVS), introduced in 1986 and revised in 1997 (and known as the Rutherford classification after the lead author, Robert B. Rutherford), consists of four grades and seven categories:[38][43]
- Grade 0, Category 0: Asymptomatic
- Grade I, Category 1: Mild claudication
- Grade I, Category 2: Moderate claudication
- Grade I, Category 3: Severe claudication
- Grade II, Category 4: Rest pain
- Grade III, Category 5: Minor tissue loss; Ischemic ulceration not exceeding ulcer of the digits of the foot
- Grade IV, Category 6: Major tissue loss; Severe ischemic ulcers or frank gangrene
The TASC (and TASC II) classification suggested PAD treatment by severity of disease seen on angiogram.[38] More recently classifications, such as the Society for Vascular Surgery "Wound, Ischemia and Foot Infection" (WIFI) classification, take into account that ischemia and angiographic disease patterns are not the only determinants of amputation risk.[44]
Moderate to severe PAD in the area of Fontaine's stage III to IV, or Rutherford's category 4 to 5, presents limb threat (risk of limb loss) in the form of critical limb ischemia.[45]
Screening
It is not clear if screening for disease is useful as it has not been properly studied.[14] This includes screening with the ankle-brachial index.[46]
Treatment
Depending on the severity of the disease, the following steps can be taken, according to the following guidelines:[47]
Lifestyle changes
- Smoking cessation (cigarettes promote PAD and are a risk factor for cardiovascular disease).
- Management of diabetes.
- Management of hypertension.
- Management of high cholesterol, and medication with antiplatelet drugs. Medication with aspirin, clopidogrel and statins, which reduce clot formation and cholesterol levels, respectively, can help with disease progression and address the other cardiovascular risks that the affected person is likely to have.
- Regular exercise for those with claudication helps open up alternative small vessels (collateral flow) and the limitation in walking often improves. Treadmill exercise (35 to 50 minutes, 3 to 4 times per week[21]) has been reviewed as another treatment with a number of positive outcomes including reduction in cardiovascular events and improved quality of life. Supervised exercise programs increase pain-free walking time and the maximum walking distance in people with PAD.
Medication
Cilostazol or pentoxifylline can improve symptoms in some.[16][48] Cilostazol may improve walking distance for people who experience claudication due to peripheral artery disease, but there is no strong evidence to suggest that it improves the quality of life, decreases mortality, or decreases the risk of cardiovascular events.[16]
Treatment with other drugs or vitamins are unsupported by clinical evidence, "but trials evaluating the effect of folate and vitamin B-12 on hyperhomocysteinemia, a putative vascular risk factor, are near completion".[47]
Revascularization
After a trial of the best medical treatment outline above, if symptoms persist, patients may be referred to a vascular or endovascular surgeon. The benefit of revascularization is thought to correspond to the severity of ischemia and the presence of other risk factors for limb loss such as wound and infection severity.[44]
- Angioplasty (PTA, or percutaneous transluminal angioplasty) can be done on solitary lesions in large arteries, such as the femoral artery, but angioplasty may not have sustained benefits.[49] Patency rates following angioplasty are highest for iliac arteries, and decrease with arteries towards the toes. Other criteria that affect outcome following revascularization are length of lesion, and number of lesions.[50][51] There does not appear to be long term advantages or sustained benefit to placing a stent following angioplasty in order to hold the narrowing of the superficial femoral artery open.[52]
- Atherectomy, in which the plaque is scraped off of the inside of the vessel wall (albeit with no better results than angioplasty).[53]
- Vascular bypass grafting can be performed to circumvent a diseased area of the arterial vasculature. The great saphenous vein is used as a conduit if available, although artificial (Gore-Tex or PTFE) material is often used for long grafts when adequate venous conduit is unavailable.
- When gangrene has set in, amputation is required to prevent infected tissues from causing sepsis, a life-threatening illness.
- Thrombolysis and thrombectomy are used in cases of arterial thrombosis or embolism.
Guidelines
An updated consensus guideline from the American College of Cardiology and American Heart Association for the diagnosis and treatment of lower extremity, renal, mesenteric and abdominal aortic PAD was compiled in 2013, combining the 2005 and 2011 guidelines.[26]
Prognosis
Individuals with PAD have an "exceptionally elevated risk for cardiovascular events and the majority will eventually die of a cardiac or cerebrovascular etiology";[54] prognosis is correlated with the severity of the PAD as measured by the ankle–brachial index.[54] Large-vessel PAD increases mortality from cardiovascular disease significantly. PAD carries a greater than "20% risk of a coronary event in 10 years".[54]
There is a low risk that an individual with claudication will develop severe ischemia and require amputation, but the risk of death from coronary events is three to four times higher than matched controls without claudication.[47] Of patients with intermittent claudication, only "7% will undergo lower extremity bypass surgery, 4% major amputations, and 16% worsening claudication", but stroke and heart attack events are elevated, and the "5-year mortality rate is estimated to be 30% (versus 10% in controls)".[54]
Epidemiology
The prevalence of peripheral artery disease in the general population is 12–14%, affecting up to 20% of those over 70;[54] 70%–80% of affected individuals are asymptomatic; only a minority ever require revascularisation or amputation. Peripheral artery disease affects 1 in 3 diabetics over the age of 50.
In the USA peripheral arterial disease affects 12–20 percent of Americans age 65 and older. Approximately 10 million Americans have PAD. Despite its prevalence and cardiovascular risk implications, only 25 percent of PAD patients are undergoing treatment.
The incidence of symptomatic PAD increases with age, from about 0.3% per year for men aged 40–55 years to about 1% per year for men aged over 75 years. The prevalence of PAD varies considerably depending on how PAD is defined, and the age of the population being studied. Diagnosis is critical, as people with PAD have a four to five times higher risk of heart attack or stroke.
The Diabetes Control and Complications Trial, and the U.K. Prospective Diabetes Study trials, in people with type 1 and type 2 diabetes, respectively, demonstrated that glycemic control is more strongly associated with microvascular disease than macrovascular disease. It may be that pathologic changes occurring in small vessels are more sensitive to chronically elevated glucose levels than is atherosclerosis occurring in larger arteries.[55]
Research
In those who have developed critically poor blood flow to the legs, it is unclear if autotransplantation of autologous mononuclear cells is useful or not.[56]
Only one randomized controlled trial has been conducted comparing vascular bypass to angioplasty for the treatment of severe PAD.[57] The trial found no difference in amputation-free survival between vascular bypass and angioplasty at the planned clinical endpoint, however the trial has been criticized as being underpowered, limiting endovascular options, and comparing inappropriate endpoints.[58] As of 2017, two randomized clinical trials are being conducted to better understand the optimal revascularization technique for severe PAD and critical limb ischemia (CLI), the BEST-CLI (Best Endovascular Versus Best Surgical Therapy for Patients With Critical Limb Ischemia) Trial, and the BASIL-2 (Bypass Versus Angio plasty in Severe Ischaemia of the Leg – 2 )Trial. [59][60]
In 2011, pCMV-vegf165 was registered in Russia as the first-in-class gene therapy drug for treatment of peripheral artery disease, including the advanced stage of critical limb ischemia.[61][62]
See also
References
- 1 2 3 4 Violi, F; Basili, S; Berger, JS; Hiatt, WR (2012). "Antiplatelet therapy in peripheral artery disease". Handbook of experimental pharmacology (210): 547–63. doi:10.1007/978-3-642-29423-5_22. PMID 22918746.
- 1 2 "What Are the Signs and Symptoms of Peripheral Arterial Disease?". nhlbi.nih.gov. August 2, 2011. Archived from the original on February 25, 2015. Retrieved February 26, 2015.
- 1 2 3 4 5 "What Is Peripheral Arterial Disease?". nhlbi.nih.gov. August 2, 2011. Archived from the original on February 25, 2015. Retrieved February 25, 2015.
- 1 2 3 "What Is Peripheral Vascular Disease?" (PDF). heart.org. 2012. Archived (PDF) from the original on April 12, 2015. Retrieved February 26, 2015.
- 1 2 "What Causes Peripheral Arterial Disease?". nhlbi.nih.gov. August 2, 2011. Archived from the original on February 25, 2015. Retrieved February 26, 2015.
- 1 2 3 4 5 Fowkes, FG; Rudan, D; Rudan, I; Aboyans, V; Denenberg, JO; McDermott, MM; Norman, PE; Sampson, UK; Williams, LJ; Mensah, GA; Criqui, MH (19 October 2013). "Comparison of global estimates of prevalence and risk factors for peripheral artery disease in 2000 and 2010: a systematic review and analysis". Lancet. 382 (9901): 1329–40. doi:10.1016/s0140-6736(13)61249-0. PMID 23915883.
- 1 2 "How Is Peripheral Arterial Disease Diagnosed?". August 2, 2011. Archived from the original on April 7, 2015. Retrieved March 27, 2015.
- 1 2 3 Ruiz-Canela, M; Martínez-González, MA (2014). "Lifestyle and dietary risk factors for peripheral artery disease". Circulation Journal. 78 (3): 553–9. doi:10.1253/circj.cj-14-0062. PMID 24492064.
- 1 2 "How Is Peripheral Arterial Disease Treated?". nhlbi.nih.gov. August 2, 2011. Archived from the original on February 25, 2015. Retrieved February 26, 2015.
- 1 2 Fokkenrood, HJ; Bendermacher, BL; Lauret, GJ; Willigendael, EM; Prins, MH; Teijink, JA (23 August 2013). "Supervised exercise therapy versus non-supervised exercise therapy for intermittent claudication". The Cochrane Database of Systematic Reviews. 8: CD005263. doi:10.1002/14651858.CD005263.pub3. PMID 23970372.
- 1 2 3 4 Hankey, GJ; Norman, PE; Eikelboom, JW (1 February 2006). "Medical treatment of peripheral arterial disease". JAMA. 295 (5): 547–53. doi:10.1001/jama.295.5.547. PMID 16449620.
- 1 2 GBD 2015 Disease and Injury Incidence and Prevalence, Collaborators. (8 October 2016). "Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990-2015: a systematic analysis for the Global Burden of Disease Study 2015". Lancet. 388 (10053): 1545–1602. doi:10.1016/S0140-6736(16)31678-6. PMC 5055577. PMID 27733282.
- 1 2 GBD 2015 Mortality and Causes of Death, Collaborators. (8 October 2016). "Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980-2015: a systematic analysis for the Global Burden of Disease Study 2015". Lancet. 388 (10053): 1459–1544. doi:10.1016/s0140-6736(16)31012-1. PMC 5388903. PMID 27733281.
- 1 2 Andras, A; Ferket, B (Apr 7, 2014). "Screening for peripheral arterial disease". The Cochrane Database of Systematic Reviews. 4: CD010835. doi:10.1002/14651858.CD010835.pub2. PMID 24711093.
- ↑ U.S. Preventive Services Task Force (December 15, 2014). "Peripheral artery disease screening and cardiovascular disease risk assessment with the ankle-brachial index in adults: recommendation statement". Am Fam Physician. 90 (12): 858A–858D. Archived from the original on March 31, 2017.
- 1 2 3 Bedenis, R; Stewart, M; Cleanthis, M; Robless, P; Mikhailidis, DP; Stansby, G (31 October 2014). "Cilostazol for intermittent claudication". The Cochrane Database of Systematic Reviews. 10: CD003748. doi:10.1002/14651858.CD003748.pub4. PMID 25358850.
- ↑ Lin, JS; Olson, CM; Johnson, ES; Whitlock, EP (3 September 2013). "The ankle-brachial index for peripheral artery disease screening and cardiovascular disease prediction among asymptomatic adults: a systematic evidence review for the U.S. Preventive Services Task Force". Annals of Internal Medicine. 159 (5): 333–41. doi:10.7326/0003-4819-159-5-201309030-00007. PMID 24026319.
- ↑ Poredos, P; Jezovnik, MK (March 2013). "Is aspirin still the drug of choice for management of patients with peripheral arterial disease?". VASA. Zeitschrift für Gefasskrankheiten. 42 (2): 88–95. doi:10.1024/0301-1526/a000251. PMID 23485835.
- ↑ Hauk, L (15 May 2012). "ACCF/AHA update peripheral artery disease management guideline". American Family Physician. 85 (10): 1000–1. PMID 22612053.
- ↑ GBD 2013 Mortality and Causes of Death, Collaborators (17 December 2014). "Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013". Lancet. 385 (9963): 117–71. doi:10.1016/S0140-6736(14)61682-2. PMC 4340604. PMID 25530442.
- 1 2 3 Peripheral Arterial Disease at Merck Manual of Diagnosis and Therapy Professional Edition. Retrieved August 9, 2010.
- 1 2 Joosten MM, Pai JK, Bertoia ML, Rimm EB, Spiegelman D, Mittleman MA, Mukamal KJ (Oct 2012). "Associations between conventional cardiovascular risk factors and risk of peripheral artery disease in men". JAMA. 308 (16): 1660–7. doi:10.1001/jama.2012.13415. PMC 3733106. PMID 23093164.
- ↑ Price J, Mowbray P, Lee A, Rumley A, Lowe G, Fowkes F (1999). "Relationship between smoking and cardiovascular risk factors in the development of peripheral arterial disease and coronary artery disease; Edinburgh Artery Study Edinburgh Artery Study". European Heart Journal. 20 (5): 344–353. doi:10.1053/euhj.1998.1194.
- ↑ Smith GD, Shipley M, Rose G (1990). "Intermittent claudication, heart disease risk factors, and mortality. The Whitehall Study". Circulation. 82 (6): 1925–1931. doi:10.1161/01.cir.82.6.1925.
- ↑ Cole C, Hill G, Farzad E, Bouchard A, Moher D, Rody K, Shea B (1993). "Cigarette smoking and peripheral arterial occlusive disease". Surgery. 114 (4): 753.
- 1 2 3 4 5 Rooke, TW; Hirsch, AT; Misra, S; Sidawy, AN; Beckman, JA; Findeiss, L; Golzarian, J; Gornik, HL; Jaff, MR; Moneta, GL; Olin, JW; Stanley, JC; White, CJ; White, JV; Zierler, RE; American College of Cardiology Foundation Task, Force; American Heart Association Task, Force (9 April 2013). "Management of patients with peripheral artery disease (compilation of 2005 and 2011 ACCF/AHA Guideline Recommendations): a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines". Journal of the American College of Cardiology. 61 (14): 1555–70. doi:10.1016/j.jacc.2013.01.004. PMC 4492473. PMID 23473760.
- ↑ Kannel WB, McGee D (1979). "Diabetes and glucose tolerance as risk factors for cardiovascular disease: the Framingham study". Diabetes Care. 2 (2): 120–126. doi:10.2337/diacare.2.2.120.
- ↑ Creager MA, Lüscher TF, Cosentino F, Beckman JA (2003). "Diabetes and vascular disease pathophysiology, clinical consequences, and medical therapy: part I." Circulation. 108 (12): 1527–1532. doi:10.1161/01.cir.0000091257.27563.32. PMC 3743069.
- ↑ Lüscher TF, Creager MA, Beckman JA, Cosentino F (2003). "Diabetes and vascular disease pathophysiology, clinical consequences, and medical therapy: Part II". Circulation. 108 (13): 1655–1661. doi:10.1161/01.cir.0000089189.70578.e2.
- ↑ Beks P, Mackaay A, De Neeling J, De Vries H, Bouter L, Heine R (1995). "Peripheral arterial disease in relation to glycaemic level in an elderly Caucasian population: the Hoorn study". Diabetologia. 38 (1): 86–96. doi:10.1007/s001250050257.
- ↑ Unit ES (2005). "Efficacy and safety of cholesterol-lowering treatment: prospective meta-analysis of data from 90 056 participants in 14 randomised trials of statins". Lancet. 366: 1267–1278. doi:10.1016/s0140-6736(05)67394-1.
- ↑ Kannel W, McGee D (1985). "Update on some epidemiologic features of intermittent claudication: the Framingham Study". Journal of the American Geriatrics Society. 33 (1): 13. doi:10.1111/j.1532-5415.1985.tb02853.x.
- ↑ Selvin E, Erlinger TP (2004). "Prevalence of and risk factors for peripheral arterial disease in the united states results from the national health and nutrition examination survey, 1999–2000". Circulation. 110 (6): 738–743. doi:10.1161/01.cir.0000137913.26087.f0.
- ↑ Hooi JD, Kester AD, Stoffers HE, Overdijk MM, van Ree JW, Knottnerus JA (2001). "Incidence of and risk factors for asymptomatic peripheral arterial occlusive disease: a longitudinal study". American Journal of Epidemiology. 153 (7): 666–672. doi:10.1093/aje/153.7.666. PMID 11282794.
- ↑ Allison MA, Denenberg JO, Criqui MH (2011). "Family History of Peripheral Artery Disease Is Associated With Prevalence and Severity of Peripheral Artery Disease". Journal of the American College of Cardiology. 58 (13): 1386–92. doi:10.1016/j.jacc.2011.06.023. PMC 3215334. PMID 21920269.
- ↑ Valentine RJ, Guerra R, Stephan P, Scoggins E, Clagett GP, Cohen J (2004). "Family history is a major determinant of subclinical peripheral arterial disease in young adults". Journal of vascular surgery. 39 (2): 351–356. doi:10.1016/j.jvs.2003.07.011.
- ↑ Ridker PM, Stampfer MJ, Rifai N (2001). "Novel risk factors for systemic atherosclerosis". JAMA: The Journal of the American Medical Association. 285 (19): 2481–2485. doi:10.1001/jama.285.19.2481.
- 1 2 3 4 5 TASC II Guidelines
* Norgren L, Hiatt WR, Dormandy JA; Hiatt; et al. (2007). "Inter-Society Consensus for the Management of Peripheral Arterial Disease (TASC II)". Eur J Vasc Endovasc Surg. 33 (Suppl 1): S1–75. doi:10.1016/j.ejvs.2006.09.024. PMID 17140820.
* Norgren L, Hiatt WR, Dormandy JA, TASC II Working Group, et al. (2007). "Inter-Society Consensus for the Management of Peripheral Arterial Disease (TASC II)". J Vasc Surg. 45 (Suppl S): S5–67. doi:10.1016/j.jvs.2006.12.037. PMID 17223489.
* Norgren L, Hiatt WR, Dormandy JA (2007). "Inter-Society Consensus for the Management of Peripheral Arterial Disease". Int Angiol. 26 (2): 81–157. PMID 17489079. - ↑ Vowden P, Vowden K (March 2001). "Doppler assessment and ABPI: Interpretation in the management of leg ulceration". Worldwide Wounds. Archived from the original on May 9, 2008. - describes ABPI procedure, interpretation of results, and notes the somewhat arbitrary selection of "ABPI of 0.8 has become the accepted endpoint for high compression therapy, the trigger for referral for a vascular surgical opinion and the defining upper marker for an ulcer of mixed aetiology"
- ↑ Leiner T, Kessels AG, Nelemans PJ, Vasbinder GB, de Haan MW, Kitslaar PE, Ho KY, Tordoir JH, van Engelshoven JM699-708; Kessels; Nelemans; Vasbinder; De Haan; Kitslaar; Ho; Tordoir; Van Engelshoven (May 2005). "Peripheral arterial disease: comparison of color duplex US and contrast-enhanced MR angiography for diagnosis". Radiology. 235 (2): 699–708. doi:10.1148/radiol.2352040089. PMID 15858107.
- ↑ Leiner, T (February 2005). "Magnetic resonance angiography of abdominal and lower extremity vasculature". Top Magn Reson Imaging. 16 (1): 21–66. doi:10.1097/01.rmr.0000185431.50535.d7. PMID 16314696.
- ↑ Fontaine R, Kim M, Kieny R; Kim; Kieny (1954). "Die chirugische Behandlung der peripheren Durchblutungsstörungen. (Surgical treatment of peripheral circulation disorders)". Helvetica Chirurgica Acta (in German). 21 (5/6): 499&ndash, 533. PMID 14366554.
- ↑ Rutherford, Robert B.; Baker, J. Dennis; Ernst, Calvin; Johnston, K. Wayne; Porter, John M.; Ahn, Sam; Jones, Darrell N. (September 1997). "Recommended standards for reports dealing with lower extremity ischemia: Revised version". Journal of Vascular Surgery. 26 (3): 517–538. doi:10.1016/S0741-5214(97)70045-4. PMID 9308598.
- 1 2 Mills JL, Sr; Conte, MS; Armstrong, DG; Pomposelli, FB; Schanzer, A; Sidawy, AN; Andros, G; Society for Vascular Surgery Lower Extremity Guidelines, Committee (January 2014). "The Society for Vascular Surgery Lower Extremity Threatened Limb Classification System: risk stratification based on wound, ischemia, and foot infection (WIfI)". Journal of vascular surgery. 59 (1): 220–34.e1-2. doi:10.1016/j.jvs.2013.08.003. PMID 24126108.
- ↑ Teraa, M; et al. (2016), "Critical limb ischemia: current trends and future directions", J Am Heart Assoc, 5 (2): e002938, doi:10.1161/JAHA.115.002938, PMC 4802465, PMID 26908409.
- ↑ US Preventive Services Task, Force.; Curry, SJ; Krist, AH; Owens, DK; Barry, MJ; Caughey, AB; Davidson, KW; Doubeni, CA; Epling JW, Jr; Kemper, AR; Kubik, M; Landefeld, CS; Mangione, CM; Silverstein, M; Simon, MA; Tseng, CW; Wong, JB (10 July 2018). "Screening for Peripheral Artery Disease and Cardiovascular Disease Risk Assessment With the Ankle-Brachial Index: US Preventive Services Task Force Recommendation Statement". JAMA. 320 (2): 177–183. doi:10.1001/jama.2018.8357. PMID 29998344.
- 1 2 3 Burns P, Gough S, Bradbury AW; Gough; Bradbury (March 2003). "Management of peripheral arterial disease in primary care". BMJ. 326 (7389): 584–8. doi:10.1136/bmj.326.7389.584. PMC 1125476. PMID 12637405.
- ↑ Salhiyyah, Kareem; Senanayake, Eshan; Abdel-Hadi, Mohammed; Booth, Andrew; Michaels, Jonathan A (2012). Salhiyyah, Kareem, ed. "Pentoxifylline for intermittent claudication". Cochrane Database of Systematic Reviews (Systematic Review). 1: CD005262. doi:10.1002/14651858.CD005262.pub2. PMID 22258961.
- ↑ Fowkes FG, Gillespie IN; Gillespie (2000). Fowkes, Gerry, ed. "Angioplasty (versus non surgical management) for intermittent claudication". Cochrane Database Syst Rev (2): CD000017. doi:10.1002/14651858.CD000017. PMID 10796469.
- ↑ Johnston KW, Rae M, Hogg-Johnston SA, Colapinto RF, Walker PM, Baird RJ, Sniderman KW, Kalman P (1987). "5-year results of a prospective study of percutaneous transluminal angioplasty". Annals of Surgery. 206 (4): 403–413. doi:10.1097/00000658-198710000-00002. PMC 1493220.
- ↑ Emmerich J (2005). "Current state and perspective on medical treatment of critical leg ischemia: gene and cell therapy". The international journal of lower extremity wounds. 4 (4): 234–241. doi:10.1177/1534734605283538.
- ↑ Chowdhury, Mohammed M.; McLain, Alexander D.; Twine, Christopher P. (2014-06-24). "Angioplasty versus bare metal stenting for superficial femoral artery lesions". The Cochrane Database of Systematic Reviews (6): CD006767. doi:10.1002/14651858.CD006767.pub3. ISSN 1469-493X. PMID 24959692.
- ↑ Ambler, GK; Radwan, R; Hayes, PD; Twine, CP (17 March 2014). "Atherectomy for peripheral arterial disease". The Cochrane Database of Systematic Reviews. 3: CD006680. doi:10.1002/14651858.CD006680.pub2. PMID 24638972.
- 1 2 3 4 5 Shammas NW (2007). "Epidemiology, classification, and modifiable risk factors of peripheral arterial disease". Vasc Health Risk Manag. 3 (2): 229–34. doi:10.2147/vhrm.2007.3.2.229. PMC 1994028. PMID 17580733.
- ↑ Selvin E, Wattanakit K, Steffes MW, Coresh J, Sharrett AR; Wattanakit; Steffes; Coresh; Sharrett (April 2006). "HbA1c and peripheral arterial disease in diabetes: the Atherosclerosis Risk in Communities study". Diabetes Care. 29 (4): 877–82. doi:10.2337/diacare.29.04.06.dc05-2018. PMID 16567831. Archived from the original on March 4, 2012.
- ↑ Moazzami, K; Moazzami, B; Roohi, A; Nedjat, S; Dolmatova, E (19 December 2014). "Local intramuscular transplantation of autologous mononuclear cells for critical lower limb ischaemia". The Cochrane Database of Systematic Reviews. 12: CD008347. doi:10.1002/14651858.CD008347.pub3. PMID 25525690.
- ↑ Adam DJ, Beard JD, Cleveland T, Bell J, Bradbury AW, Forbes JF, Fowkes FG, Gillepsie I, Ruckley CV, Raab G, Storkey H (Dec 2005). "Bypass versus angioplasty in severe ischaemia of the leg (BASIL): multicentre, randomised controlled trial". Lancet. 366: 1925–34. doi:10.1016/S0140-6736(05)67704-5. PMID 16325694.
- ↑ Conte, MS (May 2010). "Bypass versus Angioplasty in Severe Ischaemia of the Leg (BASIL) and the (hoped for) dawn of evidence-based treatment for advanced limb ischemia". Journal of vascular surgery. 51 (5 Suppl): 69S–75S. doi:10.1016/j.jvs.2010.02.001. PMID 20435263.
- ↑ Menard MT, Farber A, Assmann SF; et al. (2016). "Design and Rationale of the Best Endovascular Versus Best Surgical Therapy for Patients With Critical Limb Ischemia (BEST-CLI) Trial". J Am Heart Assoc. 5: e003219. doi:10.1161/JAHA.116.003219. PMC 5015366.
- ↑ Popplewell A, Davies H, Jarrett H; et al. (2016). "Bypass versus angio plasty in severe ischaemia of the leg - 2 (BASIL-2) trial: study protocol for a randomised controlled trial". Trials. 17: 11. doi:10.1186/s13063-015-1114-2.
- ↑ "Gene Therapy for PAD Approved". December 6, 2011. Archived from the original on September 3, 2015. Retrieved August 5, 2015.
- ↑ Deev, R.; Bozo, I.; Mzhavanadze, N.; Voronov, D.; Gavrilenko, A.; Chervyakov, Yu.; Staroverov, I.; Kalinin, R.; Shvalb, P.; Isaev, A. (13 March 2015). "pCMV-vegf165 Intramuscular Gene Transfer is an Effective Method of Treatment for Patients With Chronic Lower Limb Ischemia". Journal of cardiovascular pharmacology and therapeutics. 20: 473–82. doi:10.1177/1074248415574336. PMID 25770117. Retrieved 5 August 2015.
External links
- "Peripheral Arterial Disease" at the National Heart, Lung and Blood Institute
- Peripheral Arterial Disease (P.A.D.) at the American College of Foot and Ankle Surgeons
- Gerhard-Herman, Marie D.; Gornik, Heather L.; Barrett, Coletta; Barshes, Neal R.; Corriere, Matthew A.; et al. (13 November 2016). "2016 AHA/ACC Guideline on the Management of Patients With Lower Extremity Peripheral Artery Disease: Executive Summary". Circulation. 135: CIR.0000000000000470. doi:10.1161/CIR.0000000000000470.
| Classification | |
|---|---|
| External resources |