Pain management in children
| Pain management in children | |
|---|---|
 | |
| Classification and external resources | |
| Specialty | Pediatrics, Anesthesia, Neonatal medicine, Palliative medicine |
| ICD-10 | R52 |
| ICD-9-CM | 338 |
| DiseasesDB | 9503 |
| MedlinePlus | 002164 |
| MeSH | D010146 |
Pain management in children is the assessment and treatment of pain in infants and children. Similar to adults, a child's pain is often tied to emotional and psychological components.[1] Many of the problems that cause children pain are undertreated.[2] Untreated pain can greatly increase the chances of further complications and even death,[3] making it important to identify the cause of pain quickly.[2] Infants and children cannot readily identify pain depending on their level of development, so determining a method to intervene and treat pain is crucial at this early stage of life. Children can have significant pain related to epidermolysis bullosa, osteogenesis imperfecta, cancer, metabolic/neurologic diseases, palliative care, and sickle cell disease.[4] Evidence-based approaches to managing pain in children are described with: "Pain management practices should be based on scientific facts or agreed best practices, not on personal beliefs or opinion. The burden of proof lies with the healthcare professional, NOT the patient."[5] Unfortunately, many of the problems that cause children pain are undertreated.[2] Working with children in pain predisposes hospital caregivers to burnout and stress.[6]
Medical uses
Identifying Pain
In the past, it was believed that expression of pain in babies was reflexive, and that due to the immaturity of the infant brain the pain could not really be perceived.[7] Attempting to relieve pain in infants was considered futile because it was thought to be impossible to measure a child's pain.[8] These beliefs along with cultural concerns about opiate addiction contributed to the clinician's decision to withhold pain relief.[9] More recently, however, it was found that a person experiences pain as early as the gestational period.[10]
In 1994, responding to the need for a more useful system for describing chronic pain, the International Association for the Study of Pain (IASP) classified pain by the:
- Region of the body involved (e.g. abdomen, lower limbs),
- System in which dysfunction may be causing the pain (e.g., nervous, gastrointestinal),
- Duration and pattern of occurrence,
- Intensity and time since onset, and
- Cause.[11]
This system was criticized by Harvard professor of neurology and neurobiology Clifford J. Woolf and others as inadequate for guiding treatment.[12] Woolf suggested three categories of pain:
- Nociceptive pain,
- Inflammatory pain which is associated with tissue damage and the infiltration of immune cells, and
- Pathological pain which is a disease state caused by damage to the nervous system or by its abnormal function (e.g. fibromyalgia, peripheral neuropathy, tension type headache).[13]
Treatments can vary among health care providers according to providers' personalities, cultures, beliefs and acceptance of pain in children. Characteristics of pain typically help determine assessment, diagnosis and treatment. Pain can be acute, recurrent, chronic or a combination of these. It may occur in more than one body part simultaneously. To best assess pain in a child, the child can be asked to describe the pain before they are asked about location, intensity, quality, or tolerance. Assessing a child's pain based on the judgement of their parents or caregivers may lead to underestimation, as there is a widespread tendency for people to underestimate the pain of others.[2] The suggested treatments for pain do not always resolve the problem, and in some cases, treatments and medications for pain actually cause pain. Minor invasive procedures often do not include a treatment plan for consequent pain. For example, during circumcision infants do not consistently receive appropriate pain control. Not only are newborn circumcisions painful, they are also associated with irritability and feeding disturbances for days after the procedure.[2] The American Association of Pediatrics states pain with immunizations as being minor.[14]
Contraindications and side effects
During labor, pain control used to control pain in the laboring woman may cause respiratory depression in the infant. The use of opioids can result in a number of complications in children, including respiratory depression and risk for unintended overdose and opioid misuse later in life. These risks can be reduced by the use of ibuprofen and paracetamol. The safety of opioids in children has not been established. More side effects are associated with morphine than with ibuprofen.[15] Other side effects are constipation, fatigue, and disorientation. Children can develop opioid tolerance where larger doses are needed to have the same effect. When resistance to opioids develop, the pain responsiveness is reset and pain increases. Tolerance is likely to develop in younger children.[4] Non-pharmacological treatments have few side effects.
Indications
Acute pain
Usually, acute pain has an obvious cause and is expected to last for a few days or weeks. It is usually managed with medication and non-pharmacological treatment to provide comfort.[16][17] Acute pain is an indication for needed assessment, treatment and prevention. While a child is experiencing pain, physiological consequences can jeopardize healing and recovery. Unrelieved pain can cause alkalosis and hypoxemia that result from rapid, shallow breathing. This shallow breathing can lead to the accumulation of fluid in the lungs, taking away the ability to cough. Pain can cause an increase in blood pressure and heart rate, putting stress on the heart. Pain also increases the release of anti-inflammatory steroids that reduce the ability to fight infection, increase the metabolic rate and affect healing. Another harmful outcome of acute pain is an increase in sympathetic effects such as the inability to urinate. Pain can also slow the gastrointestinal system.
Inadequate pain management in children can lead to psycho-social consequences, including lack of interest in food, apathy, sleep problems, anxiety, avoidance of discussions about health, fear, hopelessness and powerlessness. Other consequences include extended hospital stays, high re-admission rates and longer recovery.[18]
Examples of harmful consequences of unrelieved pain include:[19]
- Infants who have had more than average heel pricks can have poor cognitive and motor function;
- Associations of needles with distress may make later medical treatments more difficult;
- Children who have experienced invasive procedures often develop post-traumatic stress;
- Boys circumcised without anesthesia were found to have greater distress than uncircumcised boys;[20]
- Severe pain as a child is associated with higher reports of pain in adults.[21]
Pain can be caused by medical procedures. Acute pain can be expected in response to many if not most invasive procedures. Anticipation of pain and distress can guide pain prevention plan before treatment based on past reports of pain associated with the medical procedure. Individuals with technical expertise and experience are more likely to minimize the pain as much as possible. Preparation before a procedure with information that is understood by children and parents decreases distress. Parents can help by learning effective methods to comfort their child.[2] Types of procedures determine the use of deep sedation or anesthesia. In some cases, the best method to prevent and relieve pain is to build self-esteem. Suggested cognitive behavioral strategies include: imagery, relaxation, massage, heat compression, calm adults, a quiet environment, and confident explanations by providers. Since distress can be addressed and controlled, some children benefit from the opportunity for self-regulation. Pain reduction during invasive procedures is closely linked to controlling distress. Distress can be treated even for minor procedures such as venipuncture.[2]
Neuropathic pain
Neuropathic pain is associated with nerve injuries or abnormal sensitivities to touch or contact. Causes include past surgeries and amputations.[4]
Cancer pain
Cancer pain is managed differently from other types of pain. Clinicians treating cancer pain can come from a variety of disciplines or specialties. Typically, each specialist obtains a medical history, performs physical examinations, and documents the age and overall health of the child. The type of cancer may influence decisions about pain management. The extent of the cancer, the tolerance of the child to specific medications, procedure or therapies is also taken into account. The preferences of the parent or caregiver contribute to the determining the best way to treat cancer pain.[17] For cancer pain, opioids are helpful and can be taken orally. Others are given IV, subcutaneous, or trans-dermal. Switching medications may be necessary at times. Dosing for children is based upon studies with adults or short-term studies. Children can develop opioid tolerance where larger doses are needed to have the same effect. When resistance to opioids develop, the pain responsiveness is reset and pain increases. Tolerance is likely to develop in younger children.[4] Cancer pain can differ from other types of pain. In addition, a child can have pain for other reasons not associated with cancer. Pain in children without cancer can present itself as headaches, muscles strains, and "as being part of being a child."[17] Pain experienced by children is related to the stage or extent of the cancer. Children with cancer may have no pain. One child may have a different threshold for pain than another. Other sources of pain from cancer are: Sources of cancer pain include:
- A growing tumor pressing on a body organ or nerves
- Inadequate blood circulation because of blocked blood vessels
- Blockage of an organ or a tube of the organ
- The spread of the cancer
- Infection
- Inflammation
- Side effects of chemotherapy, radiation treatment or surgery
- Inactivity and stiffness
- Depression and anxiety[17]
Chronic pain
Chronic pain in children is unresolved pain that affects activities of daily living and may result in a significant amount of missed school days. Chronic pain is present for long periods of time and is characterized as mild to severe.[17] Chronic pain has also been described as the pain experienced when the child reports a headache, abdominal pain, back pain, generalized pain or combination of these.[4] Chronic pain can develop from disease or injury and can occur simultaneously with acute pain. Children who experience chronic pain can have psychological effects. Caring for a child in pain may cause distress to the caregiver, may cause costs due to healthcare or lost wages from time off work, and may stop caregivers from leaving the house.
Assessment
The decision to assess and treat pain is influenced the beliefs and cultural background of the clinician. Ongoing and frequent assessment between all those involved in the treatment plan is documented in a readily accessible format - usually the patient record.[2] Assessment of pain in children depends on the cooperation and developmental stage of the child. Some children cannot assist in their assessment because they have not matured enough cognitively, emotionally, or physically.[22] The following sections list signs of distress and possible pain in children by age group:
Younger infants
- Inability to distinguish the stimulus from the pain
- Ability to exhibit a reflexive response to pain
- Expressions of pain
- Tightly closed eyes[4]
- Open mouth resembling a square rather than an oval or circle
- Eyebrows lowered and tightly drawn together
- Rigid body
- Thrashing
- Loud crying[22]
- Increase in heart rate, even while sleeping
Older infants
- Deliberate withdrawal from pain and possible guarding
- Loud crying
- Painful facial expressions[22]
Toddlers
Toddlers show signs of distress and possible pain by:
School-age children
School-age children show signs of distress and possible pain by:
- Anticipating the pain but less intensively, (understands concepts of time, i.e., imminent vs future pain)
- Stalling, trying to talk out of the situation where pain is anticipated
- Having muscular rigidity[22]
Adolescent
Adolescents show signs of distress and possible pain:
- With muscle tension, but with control
- With verbal expressions and descriptions[22]
Quantitative pain assessment
Although pain is subjective and can occur in a continuous spectrum of intensities, there are assessment tools that compare pain levels over time. This kind of assessment incorporates pain scales and requires a high enough developmental level for the child to respond to questions.[22] A verbal response is not always necessary to quantify pain.
Pain scales
A pain scale measures a patient's pain intensity and other features. Pain scales can be based on observational (behavioral) or physiological data, as well as self-report. Self-report is considered primary and should be obtained if possible. Pain measurements help determine the severity, type, and duration of pain. They are also used in diagnosis, to determine a treatment plan, and to evaluate the effectiveness of treatment. Pain scales are available for neonates, infants, children, adolescents, adults, seniors, and persons with impaired communication. Pain assessments are often regarded as "the 5th vital sign".[23]
| Self-report | Observational | Physiological | |
|---|---|---|---|
| Infant | — | Premature Infant Pain Profile; Neonatal/Infant Pain Scale | — |
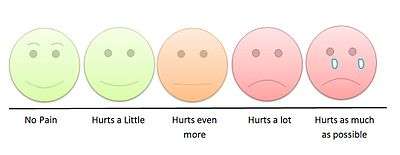
| Child | Wong-Baker Faces Pain Rating Scale – Revised;[24] Coloured Analogue Scale[25] | FLACC (Face Legs Arms Cry Consolability Scale); CHEOPS (Children's Hospital of Eastern Ontario Pain Scale)[26] | Comfort |
| Adolescent | Visual Analog Scale (VAS); Verbal Numerical Rating Scale (VNRS); Verbal Descriptor Scale (VDS); Brief Pain Inventory | — | — |
Causes
The causes of pain in children are similar to the causes in adults.
Pain can be experienced in many ways and depends on the following factors in each child:
- Prior painful episodes or treatments
- Age and developmental stage
- Disease or type of trauma
- Personality
- Culture
- Socioeconomic status
- Presence of family members and family dynamics.[22]
Misconceptions
The indications that treatment is needed are not always clear for children because of poor assessments and the tendency to undertreat pain..
| Incorrect | Valid | References |
|---|---|---|
| Infants cannot sense pain like adults | Nerve pathways exist at birth, albeit immature Newborns experience physiological changes and surges in hormones that indicate stress | [27][2] |
| Infants cannot feel pain because their nerve fibers are not myelinated | Complete myelination is not necessary for the transmission of pain impulses to the brain | [27] |
| Young children cannot indicate where pain originates | Young children may have the cognitive ability to use a body chart and explain where their pain is coming from | [27] |
| A child able to sleep must not be in pain | Sleep occurs because of exhaustion | [28] |
| "Pain builds character" | Unacceptable | [2] |
During treatment

Clinicians responsible for a child monitor the child frequently in tertiary care centers (hospitals). Pharmacological and non-pharmacological treatments are used to manage the pain. Parents or caregivers are also requested to provide their own pain assessments. At the beginning of pharmacological treatment, clinicians monitor the child for adverse reactions to the medications. The levels of some medications are monitored to ensure that the child is not over-medicated and does not receive toxic levels of any drug. The levels also indicate whether there would be enough drug in the blood to be effective in managing the pain. Medications are metabolized differently between children of the same age. Factors that influence the levels of medications controlling pain include the height, weight, and body surface of the child, as well as any other illnesses.[22] Some medications may have a paradoxical effect in children, which is an effect that is the opposite of the expected effect. Clinicians monitor for this and any other reactions to medication.[29][30]
After treatment
Post-procedural treatment in children is primarily prescription opioids, however, alternative interventions have slowly been introduced to adolescents.
Different treatment options include:
- Participation in focus groups
- Group and individual therapy
- Classes structured around living with chronic pain
All of these are examples of mindfulness-based interventions, which are currently being explored as alternatives to pharmacotherapy. These interventions explore different ways for children and adolescents to manage pain and relieve emotional distress without relying on opioids.[31] However, other interventions include medications classified as non-opioid analgesics, which are useful in post surgical treatment.[32]
Atraumatic measures
Because children process information differently from adults, treatment centers for children often use atraumatic measures to reduce anxiety and stress. Examples include:
- Allowing the parent or caregiver to be present for painful procedures
- Using a treatment room for painful procedures to ensure that the child's room is a place where little pain can be expected
- Establishing other "pain-free zones" where no medical procedures are allowed, such as a playroom
- Offering choices to the child to give them some control over the procedures
- Modelling procedures with dolls and toys
- Using age-appropriate anatomical terms and other vocabulary.[22]
Non-pharmacological pain management
Non-pharmacological methods to manage discomfort during immunizations include putting sugar on a pacifier, comforting the child during and after the injection, chest-to-chest hugging, and letting the child choose the injection site.[14] Other non-pharmacological treatments that have been found to be effective include:
- Carefully explaining a procedure with pictures or other visual aids
- Allowing the child to ask questions of medical staff
- Touring the place where the procedures will occur
- Allowing small children to play with dolls or other toys with a clinician to understand the procedure
- Allowing older children to watch a video that explains the procedure
- Providing distraction with songs, stories, toys, color, videos, TV, or music
- Using relaxation techniques such as deep breathing or massages[17]
Non-pharmacological treatment for pain associated with venipuncture in children includes hypnosis and distraction. These treatments reduced self-reported pain and when combined with cognitive-behavioural therapy (CBT) the reduction of pain was even greater. Other interventions have not been found to be effective and these are suggestion, blowing out air, and distraction with parent coaching did not differ from control for pain and distress[33][17]
Breastfeeding during painful procedures has been found to be more effective in controlling pain than placebo or positioning. Breastmilk or 'sugar' water has a similar effect, though studies in preterm infants have yet to be done.[34] Skin-to-skin care (kangaroo care) is thought be effective for pain control during painful procedures.[35][36]
Pharmacotherapy
Acute pain, chronic pain, neuropathic pain and recurrent pain in children is most often managed with medication. Most of these medications are analgesics. These include acetaminophen, NSAIDs, local anesthetics, opioids, and medications for neuropathic pain.[4] The most effective approach to pain management in children is to provide pain control around the clock instead of providing pain relief as needed. Regional anesthesia is also effective and recommended whenever possible. Opioids are effective too but often depress breathing in infants.[4] Recent evidence-based studies indicate that morphine is not superior to ibuprofen for managing children’s pain after some surgical procedures.[15] A needle-free powder lignocaine delivery system has been shown to decrease the pain of venipuncture in children.[37][38]
Chronic pain treatment
Chronic pain is treated with a variety of medications and non-pharmacological interventions. The American Association of Pediatrics has suggested that parents be educated about providing round-the-clock medication after their children receive surgery.[39] Opioid tolerance and withdrawal can be seen in the neonatal and pediatric intensive care units. Other side effects of opioid use can include cognition deficits, altered mood, and disturbances of endocrine development. Opioid misuse can occur in adolescents and is associated with the use of alcohol, cigarettes and marijuana.[4]
Non-pharmacological treatment for children to help relieve periodic pain includes counselling and behavior modification therapy.[4]
Acute pain treatment
For acute pain, multiple medications given at the same time is proven to be most effective. This results in lower pain scores, provides greater relief, allows lower dosing and side effects, targets different nerve pathways, and can be tailored to the child.[40][4]
Cancer pain treatment
Cancer pain is managed differently in children. Clinicians treating cancer pain can come from a variety of disciplines or specialities. Typically, medical history, physical examinations, age and overall health of the child are evaluated. The type of cancer may influence decisions about pain management. The extent of the cancer, and the tolerance of the child to specific medications, procedures or therapies are also taken into account, as well as the preferences of the parent or caregiver.[17] Opioids are helpful for cancer pain and can be taken orally. The side effects are constipation, fatigue, and disorientation. Others children are given intravenous injection, either subcutaneous or trans-dermal. Switching medications may be necessary at times. Dosing for children is based upon studies with adults or short-term studies. Children can develop opioid tolerance where larger doses are needed to have the same effect. When resistance to opioids develops, the pain responsiveness is reset and pain increases. Tolerance is likely to develop in younger children.[4]
Pharmacotherapy abuse
Over the past 30 years, opioid prescription rates for pain management treatment in children and adolescents have increased by almost 50% across the United States.[41] Currently, the rates of reported pain remain steady, but abuse and subsequent teen death rates have risen.[42]
The number one way teens obtain opioids is from a previous prescription or from a friend or relative with an opioid prescription, however other routes of obtaining opioids include:
- Stealing from a friend or relative,
- Purchasing from a friend of relative, and
- Purchasing illegally[32]
To combat the opioid epidemic, interventions have been taken across the United States. Collection centers for unused opioids and medications have been created as well as protocols for disposing of opioids appropriately so that they do not recycle back into the community.[43] Most law enforcement offices contain a drop box for opioids with a no questions asked policy. A large force in preventing abuse of opioids is social media which has detected illegal sales of opioids in recent years.[44]
In culture
The control of pain in children is thought to be an ethical 'imperative'.[17] The undertreatment of the pain in children has been a 'global concern' for some time. Those who have been critics of controlling pain in children have been criticized by others: "Effective pain management...involves an interdisciplinary therapeutic approach with a combination of pharmacologic, cognitive-behavioral, psychologic, and physical treatments."[2] Cultures that value stoicism may discount the pain experienced by children.[2] Greater than 60% of children are prescribed an opiate after outpatient treatment in the US.[15]
References
- ↑ "Medical Definition of Pain". Retrieved 15 August 2017.
- 1 2 3 4 5 6 7 8 9 10 11 12 Health, Committee on Psychosocial Aspects of Child and Family; Task Force on Pain in Infants, Children (1 September 2001). "The Assessment and Management of Acute Pain in Infants, Children, and Adolescents". Pediatrics. 108 (3): 793–797. doi:10.1542/peds.108.3.793. PMID 11533354 – via pediatrics.aappublications.org.
- ↑ Verghese, Susan T; Hannallah, Raafat S (15 July 2010). "Acute pain management in children". Journal of Pain Research. 3: 105–123. PMC 3004641. PMID 21197314.
- 1 2 3 4 5 6 7 8 9 10 11 12 Berde, Charles. "Pharmacotherapy of Pain in Infants and Children" (PDF). Food and Drug Administration. Retrieved 18 August 2017.
- ↑ Twycross, p. 13.
- ↑ Colville, Gillian (2018-01-01). "Paediatric intensive care nurses report higher empathy but also higher burnout than other health professionals". Evidence-Based Nursing. 21 (1): 25–25. doi:10.1136/eb-2017-102774. ISSN 1367-6539. PMID 29025856.
- ↑ Chamberlain DB (1989). "Babies Remember Pain". Pre- and Peri-natal Psychology. 3 (4): 297–310.
- ↑ Wagner AM (July 1998). "Pain control in the pediatric patient". Dermatol Clin. 16 (3): 609–17. doi:10.1016/s0733-8635(05)70256-4. PMID 9704215.
- ↑ Mathew PJ, Mathew JL (2003). "Assessment and management of pain in infants". Postgraduate Medical Journal. 79 (934): 438–443. doi:10.1136/pmj.79.934.438. PMC 1742785. PMID 12954954.
- ↑ Mazur, Artur (2013). "Pain management in children" (PDF). Annual Agriculture Environmental Medicine. 1: 28–34.
- ↑ Classification of Chronic Pain. 2 ed. Seattle: International Association for the Study of Pain; 1994. ISBN 0-931092-05-1. p. 3 & 4.
- ↑ Towards a mechanism-based classification of pain?. Pain. 1998;77(3):227–9. doi:10.1016/S0304-3959(98)00099-2. PMID 9808347.
- ↑ What is this thing called pain?. Journal of Clinical Investigation. 2010;120(11):3742–4. doi:10.1172/JCI45178. PMID 21041955.
- 1 2 "Managing Your Child's Pain While Getting a Shot". HealthyChildren.org. Retrieved 20 August 2017.
- 1 2 3 Groenewald, Cornelius Botha (2018-03-06). "Morphine is not superior to ibuprofen for managing children's pain following minor orthopedic surgery". Evidence-Based Nursing: ebnurs–2017–102855. doi:10.1136/eb-2017-102855. ISSN 1367-6539. PMID 29514849.
- ↑ Twycross, p. 140.
- 1 2 3 4 5 6 7 8 9 "Pain Management and Children". Stanford University School of Medicine, Stanford Children's Health. 2017. Retrieved 20 August 2017.
- ↑ Twycross, p. 3.
- ↑ Twycross, p. 1.
- ↑ twycross, p. 3.
- ↑ Twycross, p. 2.
- 1 2 3 4 5 6 7 8 9 10 Henry, p. 43.
- ↑ "Pain: current understanding of assessment, management and treatments" (PDF). Joint Commission on Accreditation of Healthcare Organizations andnthe National Pharmaceutical Council, Inc. December 2001. Retrieved 2018-01-25.
- ↑ "The Faces Pain Scale – Revised". Pediatric Pain Sourcebook of Protocols, Policies and Pamphlets. 7 August 2007.
- ↑ Stinson, JN; Kavanagh, T; Yamada, J; Gill, N; Stevens, B (November 2006). "Systematic review of the psychometric properties, interpretability and feasibility of self-report pain intensity measures for use in clinical trials in children and adolescents". Pain. 125 (1–2): 143–57. doi:10.1016/j.pain.2006.05.006. PMID 16777328.
- ↑ von Baeyer, C.L.; Spagrud, L.J. (2007). "Systematic review of observational (behavioral) measures of pain for children and adolescents aged 3 to 18 years". Pain. 127 (1–2): 140–150. doi:10.1016/j.pain.2006.08.014. PMID 16996689.
- 1 2 3 Twycross, p. 7.
- ↑ Twycross & page 7.
- ↑ Moon, Young Eun (2013). "Paradoxical reaction to midazolam in children". Korean Journal of Anesthesiology. 65 (1): 2. doi:10.4097/kjae.2013.65.1.2. ISSN 2005-6419.
- ↑ Mancuso, Carissa E.; Tanzi, Maria G.; Gabay, Michael (2004). "Paradoxical Reactions to Benzodiazepines: Literature Review and Treatment Options". Pharmacotherapy. 24 (9): 1177–1185. doi:10.1592/phco.24.13.1177.38089. ISSN 0277-0008.
- ↑ Ruskin, Danielle; Harris, Lauren; Stinson, Jennifer; Kohut, Sara; Walker, Katie; McCarthy, Erinn (15 December 2017). ""I Learned to Let Go of My Pain". The Effects of Mindfulness Meditation on Adolescents with Chronic Pain: An Analysis of Participants' Treatment Experience". Children. 4 (12): 110. doi:10.3390/children4120110. PMC 5742755. PMID 29244734.
- 1 2 White, Paul F. (November 2005). "The Changing Role of Non-Opioid Analgesic Techniques in the Management of Postoperative Pain". Anesthesia & Analgesia. 101 (5S): S5. doi:10.1213/01.ANE.0000177099.28914.A7. ISSN 0003-2999.
- ↑ Ltd, BMJ Publishing Group Ltd and RCN Publishing Company (2007-07-01). "Review: distraction, hypnosis, and combined cognitive-behavioural interventions reduce needle related pain and distress in children and adolescents". Evidence-Based Nursing. 10 (3): 75–75. doi:10.1136/ebn.10.3.75. ISSN 1367-6539. PMID 17596380.
- ↑ Shah, Prakeshkumar S; Herbozo, Cecilia; Aliwalas, Lucia Liz; Shah, Vibhuti S (2012-12-12). Cochrane Database of Systematic Reviews. John Wiley & Sons, Ltd. doi:10.1002/14651858.cd004950.pub3.
- ↑ Johnston, Celeste; Campbell-Yeo, Marsha; Disher, Timothy; Benoit, Britney; Fernandes, Ananda; Streiner, David; Inglis, Darlene; Zee, Rebekah (2017). "Skin-to-skin care for procedural pain in neonates". The Cochrane Database of Systematic Reviews. 2: CD008435. doi:10.1002/14651858.CD008435.pub3. ISSN 1469-493X. PMID 28205208.
- ↑ Cong, Xiaomei (2017-10-01). "Skin-to-skin care is an effective and safe intervention to reduce procedural pain in neonates". Evidence-Based Nursing. 20 (4): 113–113. doi:10.1136/eb-2017-102684. ISSN 1367-6539. PMID 28739607.
- ↑ Lacroix, Helene (2008-10-01). "A needle-free powder lignocaine delivery system reduced the pain of venipuncture in childrenCommentary". Evidence-Based Nursing. 11 (4): 106–106. doi:10.1136/ebn.11.4.106. ISSN 1367-6539. PMID 18815318.
- ↑ Ltd, BMJ Publishing Group Ltd and RCN Publishing Company (2006-01-01). "Liposomal lidocaine improved intravenous cannulation success rates in children". Evidence-Based Nursing. 9 (1): 10–10. doi:10.1136/ebn.9.1.10. ISSN 1367-6539. PMID 16437788.
- ↑ Fortier, Michelle A.; MacLaren, Jill E.; Martin, Sarah R.; Perret-Karimi, Danielle; Kain, Zeev N. (1 October 2009). "Pediatric Pain After Ambulatory Surgery: Where's the Medication?". Pediatrics. 124 (4): e588–e595. doi:10.1542/peds.2008-3529. PMID 19736260. Retrieved 20 August 2017 – via pediatrics.aappublications.org.
- ↑ Twycross, p. 147.
- ↑ Mazer-Amirshahi, Maryann (2014). "Trends in prescription opioid use in pediatric emergency department patients". Pediatric Emergency Care. 30: 230–235. doi:10.1097/pec.0000000000000102 – via Medline.
- ↑ "Prescribing Data | Drug Overdose | CDC Injury Center". www.cdc.gov. 2017-08-31. Retrieved 2018-03-14.
- ↑ "End the Opioid Epidemic". End the Opioid Epidemic. Retrieved 2018-03-22.
- ↑ "Opioid epidemic". Wikipedia. 2018-03-21.
Bibliography
- Henry, Norma (2016). RN nursing care of children : review module. Stilwell, KS: Assessment Technologies Institute. ISBN 9781565335714.
- Roberts, Michael (2017). Handbook of pediatric psychology. New York: The Guilford Press. ISBN 9781462529780.
- Twycross, Alison (2014). Managing pain in children : a clinical guide for nurses and healthcare professionals. Hoboken: Wiley Blackwell. ISBN 9780470670545.