Glenoid labrum
| Glenoidal labrum | |
|---|---|
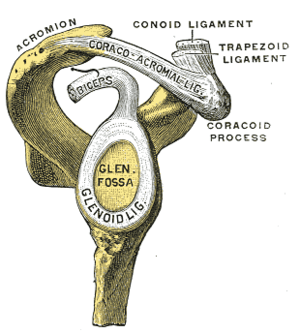 Lateral view of the shoulder showing the glenoid labrum (marked "glenoid ligament") | |
| Details | |
| Identifiers | |
| Latin | labrum glenoidale |
| TA | A03.5.08.002 |
| FMA | 23290 |
| Anatomical terminology | |
The glenoid labrum (glenoid ligament) is a fibrocartilaginous structure (not a fibrocartilage as previously thought) rim attached around the margin of the glenoid cavity in the shoulder blade. The shoulder joint is considered a ball and socket joint. However, in bony terms the 'socket' (the glenoid fossa of the scapula) is quite shallow and small, covering at most only a third of the 'ball' (the head of the humerus). The socket is deepened by the glenoid labrum.
The labrum is triangular in section; the base is fixed to the circumference of the cavity, while the free edge is thin and sharp.
It is continuous above with the tendon of the long head of the biceps brachii, which gives off two fascicles to blend with the fibrous tissue of the labrum.
Structure
Clinical significance
Injury
Tearing of the labrum can occur from either acute trauma or repetitive shoulder motion such as in the sports of swimming, baseball and football. Acute trauma may be from dislocation of the shoulder, direct blows to the shoulder, and other accidents of the sort. Tears are classified as either superior or inferior in regards to where the tear is in the glenoid cavity. A SLAP lesion (superior labrum, anterior to posterior) is a tear where the glenoid labrum meets the tendon of the long head of the biceps muscle. Symptoms include increased pain with overhead activity, popping or grinding, loss of strength, and trouble localizing a specific point of pain. Because a SLAP lesion involves the biceps, pain and weakness may also be felt when performing elbow flexion with resistance.
Diagnosis
Clinicians can use any combination of the following manual tests to assist in determining if a labral tear has occurred; Jobe Relocation, O'Brien, Anterior Apprehension, Bicipital Groove Tenderness, Crank, Speed, and Yergason tests. As a general rule, abnormal pain experienced during any of these tests will indicate a positive result, or a tear of the glenoid labrum. All of the tests take advantage of the fact that the labrum meets the tendon of the long head of the biceps muscle and thus will normally produce pain in the region if a tear is present. Additionally clinicians may order an MRI (Magnetic Resonance Imaging) or CT (Computed Tomography) scan to be conducted utilizing contrast injections to highlight where tears may be present. However; due to inherent variability between humans, manual tests, when possible, are more accurate in determining the presence of a labral tear.[1]
See also
References
This article incorporates text in the public domain from page 319 of the 20th edition of Gray's Anatomy (1918)
- ↑ Guanche, C. "Clinical Testing for Tears of the Glenoid Labrum" (PDF). Retrieved 28 November 2016.
External links
| Wikimedia Commons has media related to Glenoid labrum. |
- upper%20extremity/arthrogramaxial2 at the Dartmouth Medical School's Department of Anatomy
- http://orthoinfo.aaos.org/topic.cfm?topic=a00426
- https://web.archive.org/web/20121119012737/http://www.orthospecmd.com/SLAPlesion.html
- http://www.carlosguanchemd.com/wp-content/uploads/2012/08/Clinical-Testing-for-Tears-of-the-Glenoid-Labrum.pdf