Dental dam
A dental dam or rubber dam (sometimes termed "Kofferdam"—from German), designed in the United States in 1864 by Sanford Christie Barnum,[1] is a thin, 6-inch (150 mm) square sheet, usually latex or nitrile, used in dentistry to isolate the operative site (one or more teeth) from the rest of the mouth. It is used mainly in endodontic, fixed prosthodontic (crowns, bridges) and general restorative treatments. Its purpose is both to prevent saliva interfering with the dental work (e.g. contamination of oral micro-organisms during root canal therapy, or to keep filling materials such as composite dry during placement and curing), and to prevent instruments and materials from being inhaled, swallowed or damaging the mouth. In dentistry, use of a rubber dam is sometimes referred to as isolation.[2]
Dental dams may also be used as a safe sex technique to reduce the risk of sexually transmitted infections (STIs) during cunnilingus and other sexual activities.
Dentistry

Background
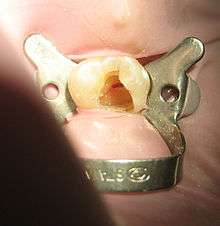
The dam is held over individual teeth or groups of teeth by appropriate rubber dam clamps over the anchor tooth. The tooth crown stands out from the rubber dam through individual holes made by a hole punch, isolating the tooth to be treated from the rest of the person's mouth which keeps the tooth dry and reduces risk of exposure to oral micro-organisms. An ink stamp is available to guide placement of the holes prior to application of the dam.[3]
Advantages
- Clean and dry operating field (saliva, blood). For dentistry procedures involving bonding with adhesives or cements it is to be encouraged as the operative field must avoid contamination in order to achieve maximum bond strength between restorative material, enamel and dentin. Poor bonding may compromise the success or longevity of the restorations. There is some evidence to suggest that the use of a rubber dam may increase the survival time of dental restorations compared to the use of cotton rolls as an isolation method.[4]
- Decreased contamination of dental treatment with oral micro-organisms in saliva[5]
- There is improved visibility of the operative site (retracts the lips and cheeks, reduced mirror fogging, enhanced visual contrast)[6]
- Decreased (but not eliminated) chance of accidental swallowing or inhaling restorative instruments, tooth fragments or debris.[7] Should this occur, hospital admission might be necessary for a chest x-ray, and potentially an operation to remove it.
- Corrosive endodontic irrigants such as sodium hypochlorite (bleach) are contained, which could damage the soft tissues of the mouth and be harmful if swallowed[8]
- Reduction in the risk of cross-infection in the dental practice by decreasing the microbial content of splatters and air turbine aerosols produced during dental treatment[9]
- When rubber dams are used in association with amalgam restorations, they may reduce the person's exposure to potentially harmful adverse effects of mercury ingestion[10][11]
- Protecting soft tissues of oral mucosa from sharp instruments or materials. A caulking adhesive is sometimes used to fill in the gaps between the rubber dam and gingiva. It can adhere to wet rubber dam, or mucosal tissues [12].
 Sealing agent used on a patient to fill in some gaps between the rubber dam and gingiva, after a tear was caused in the rubber dam
Sealing agent used on a patient to fill in some gaps between the rubber dam and gingiva, after a tear was caused in the rubber dam - Some patients find it more comfortable to have treatment with a dental dam since there is no water in the mouth and they feel safer and more dissociated from the noise of drilling etc.[13]
- In some parts of the world, use of a dental dam is mandatory for procedures such as root canal therapy for reasons of safety and cross infection control, and if any injury that could have been prevented by its use occurs, it is medicolegally indefensible.
- The dental dam significantly reduces the ability of the dental patient to communicate. This can be considered a disadvantage (see below), or an advantage, e.g. in over-talkative patients to facilitate faster treatment
- A Cochrane review in 2016 suggested that on using rubber dam as an isolation method, there's a chance dental restorations last longer [14].
Disadvantages
- It takes extra time to apply (although with practice this becomes fast)
- Insufficient training and inconvenience[15]
- The cost of dental dams and the kit to apply it. Although not expensive, this cost would not be incurred if it was not used
- Rubber dam clamps may break during dental treatments due to effect of sodium hypochlorite or autoclaving.[16] As a precaution, place floss around clamp to allow its retrieval if it flies off or breaks during a procedure.
- Damage to the oral mucosa when placing or removing the rubber dam.
- Since it effectively blocks off the oral airway, the patient must be able to comfortably breathe through their nose. Of relevance are temporary causes of nasal airway obstruction such as the common cold, or persons who continually breathe through their mouth for whatever reason.
- To an extent, it may lead to visual distortion of tooth morphology since the other teeth and the rest of the mouth are hidden from view. This may lead to perforation if an access cavity is incorrectly angled during root canal therapy. For this reason, some endodontists routinely begin their access cavity before applying the dam, to ensure the correct orientation before the root canal system is opened up.
- The dam, which is usually brightly colored (blue or green), may alter the apparent color of the tooth, which can lead to incorrect choice of shade, e.g. during placement of a dental composite. For this reason, shades are normally chosen before the dam is applied.
- Latex allergy, depending upon the severity, may make the use of rubber dam uncomfortable afterwards (allergic contact dermatitis, allergic contact cheilitis, allergic contact stomatitis) or even life-threatening (anaphylaxis). Nitrile versions are available for those with latex allergies, however this type of dam is more stretchy, therefore a smaller size of hole should be punched in the dam.
- Some patients find the dental dam claustrophobic.
- Reduced communication between patient and dentist may increase patient anxiety and make them feel more vulnerable.
Safe sex
Sometimes dental dams are promoted during safe sex campaigns, for use during cunnilingus and anilingus, especially for women who have sex with women.[17][18] However, they are rarely used by women who have sex with women for this purpose,[17][19][20] and there is no good evidence that their use reduces the risk of STI transmission in this group, including the risk of infection with human immunodeficiency virus.[20] After lubrication with a water-based lubricant, an unpunctured dental dam may be held over the vulva or anus, allowing oral stimulation of these areas without transmission of bodily fluids and direct physical contact. Condoms can be turned into dental dams by cutting the condom open.[21]
References
- ↑ Elderton, R. J. (1971-02-01). "A modern approach to the use of rubber dam--1". The Dental Practitioner and Dental Record. 21 (6): 187–193. ISSN 0011-8729. PMID 5278933.
- ↑ Luca Martinelli, The rubber dam technique, Academia.
- ↑ Bun San Chong, Shanon Patel, Bhavin Bhuva, Rubber dam in clinical practice, ENDO (Lond Engl) 2008;2(2):131–141.
- ↑ Wang, Yan; Li, Chunjie; Yuan, He; Wong, May CM; Zou, Jing; Shi, Zongdao; Zhou, Xuedong (2016-09-20). Cochrane Database of Systematic Reviews. John Wiley & Sons, Ltd. doi:10.1002/14651858.cd009858.pub2. ISSN 1465-1858.
- ↑ Cochran, M. A.; Miller, C. H.; Sheldrake, M. A. (1989-07-01). "The efficacy of the rubber dam as a barrier to the spread of microorganisms during dental treatment". Journal of the American Dental Association (1939). 119 (1): 141–144. ISSN 0002-8177. PMID 2760346.
- ↑ Reid JS, Callis PD, Patterson CJ (1991). Rubber Dam in Clinical Practice (1st ed.). London: Quintessence Publishing.
- ↑ Tiwana, Karen K.; Morton, Teresa; Tiwana, Paul S. (2004-09-01). "Aspiration and ingestion in dental practice: a 10-year institutional review". Journal of the American Dental Association (1939). 135 (9): 1287–1291. ISSN 0002-8177. PMID 15493393.
- ↑ Cohen, S.; Schwartz, S. (1987-04-01). "Endodontic complications and the law". Journal of Endodontics. 13 (4): 191–197. doi:10.1016/S0099-2399(87)80139-5. ISSN 0099-2399. PMID 3471843.
- ↑ Harrel, Stephen K.; Molinari, John (2004-04-01). "Aerosols and splatter in dentistry: a brief review of the literature and infection control implications". Journal of the American Dental Association (1939). 135 (4): 429–437. ISSN 0002-8177. PMID 15127864.
- ↑ Kremers, L.; Halbach, S.; Willruth, H.; Mehl, A.; Welzl, G.; Wack, F. X.; Hickel, R.; Greim, H. (1999-06-01). "Effect of rubber dam on mercury exposure during amalgam removal". European Journal of Oral Sciences. 107 (3): 202–207. ISSN 0909-8836. PMID 10424384.
- ↑ Halbach, S.; Vogt, S.; Köhler, W.; Felgenhauer, N.; Welzl, G.; Kremers, L.; Zilker, T.; Melchart, D. (2008-05-01). "Blood and urine mercury levels in adult amalgam patients of a randomized controlled trial: interaction of Hg species in erythrocytes" (PDF). Environmental Research. 107 (1): 69–78. doi:10.1016/j.envres.2007.07.005. ISSN 0013-9351. PMID 17767927.
- ↑ "OraSeal*". CLINICAL RESEARCH DENTAL. Retrieved 2018-05-27.
- ↑ Stewardson, D. A.; McHugh, E. S. (2002-10-01). "Patients' attitudes to rubber dam". International Endodontic Journal. 35 (10): 812–819. ISSN 0143-2885. PMID 12406374.
- ↑ Wang, Yan; Li, Chunjie; Yuan, He; Wong, May CM; Zou, Jing; Shi, Zongdao; Zhou, Xuedong (2016-09-20). "Rubber dam isolation for restorative treatment in dental patients". Cochrane Database of Systematic Reviews. doi:10.1002/14651858.CD009858.pub2. ISSN 1465-1858.
- ↑ Hill, Edward E.; Rubel, Barry S. (2008-10-01). "Do dental educators need to improve their approach to teaching rubber dam use?". Journal of Dental Education. 72 (10): 1177–1181. ISSN 0022-0337. PMID 18923098.
- ↑ Sutton, J.; Saunders, W. P. (1996-09-01). "Effect of various irrigant and autoclaving regimes on the fracture resistance of rubber dam clamps". International Endodontic Journal. 29 (5): 335–343. ISSN 0143-2885. PMID 9206417.
- 1 2 Richters, J; Prestage, G; Schneider, K; Clayton, S (Jun 2010). "Do women use dental dams? Safer sex practices of lesbians and other women who have sex with women". Sexual health. 7 (2): 165–9. doi:10.1071/SH09072. PMID 20465981.
- ↑ "Dental Dams | Sexually Transmitted Infections | Adults | sexualityandu.ca - Your Link to Sexual Well-Being". sexualityandu.ca. 2006-12-15. Retrieved 2010-09-12.
- ↑ Yap, L; Richters, J; Butler, T; Schneider, K; Kirkwood, K; Donovan, B (Jun 2010). "Sexual practices and dental dam use among women prisoners--a mixed methods study". Sexual health. 7 (2): 170–6. doi:10.1071/SH09138. PMID 20465982.
- 1 2 Jonathan Zenilman, Mohsen Shahmanesh (2012). Sexually transmitted infections : diagnosis, management, and treatment. Sudbury, Mass.: Jones & Bartlett Learning. p. 330. ISBN 9780763786755.
- ↑ "Dental Dam Use". www.cdc.gov. Centers for Disease Control and Prevention. Retrieved 2018-09-18.