Causes and origins of Tourette syndrome
Causes and origins of Tourette syndrome have not been fully elucidated. Tourette syndrome (also called "Tourette's syndrome", "Tourette's disorder", "Gilles de la Tourette syndrome", "GTS" or "TS") is an inherited neurological disorder with onset in childhood, characterized by the presence of multiple motor tics and at least one phonic tic, which characteristically wax and wane. Tourette's syndrome occurs along a spectrum of tic disorders, which includes transient tics and chronic tics.[1][2]
The exact cause of Tourette's is unknown, but it is well established that both genetic and environmental factors are involved.[3] The overwhelming majority of cases of Tourette's are inherited, although the exact mode of inheritance is not yet known,[4] and no gene has been identified.[5] Tics are believed to result from dysfunction in the thalamus, basal ganglia, and frontal cortex of the brain,[3] involving abnormal activity of the brain chemical, or neurotransmitter, dopamine. In addition to dopamine, multiple neurotransmitters, like serotonin, GABA, glutamate, and histamine (H3-receptor), are involved.[6]
Non-genetic factors—while not causing Tourette's—can influence the severity of the disorder. Some forms of Tourette's may be genetically linked to obsessive-compulsive disorder (OCD), while the relationship between Tourette's and attention-deficit hyperactivity disorder (ADHD) is not yet fully understood.
Genetic factors
Genetic studies, including twin studies,[7] have proven that the overwhelming majority of cases of Tourette syndrome are inherited, although the exact mode of inheritance is not yet known.[8] Tic disorders have long been thought to be inherited as an autosomal dominant gene, but recent research challenges the autosomal dominant hypothesis, and suggests an additive model involving multiple genes.[5][9] According to Roger Freeman, MD, "Genes that cause tics have not yet been identified; it's very unlikely there's just one. Tics are very familial, but not in a Mendelian pattern (dominant, recessive, etc.). You can't 'inherit' the committee decision to define a problem in a specific way, so TS itself can't be inherited. It's a tic disorder that is inherited."[10]
In some cases, tics may not be inherited; these cases are identified as "sporadic" Tourette syndrome (also known as tourettism) because a genetic link is missing.[11]
A person with Tourette syndrome has about a 50% chance of passing the gene(s) to one of his/her children. Gender appears to have a role in the expression of the genetic vulnerability, with males more likely to express tics than females.[5] Tourette syndrome is a condition of incomplete penetrance, meaning not everyone who inherits the genetic vulnerability will show symptoms. Tourette's also shows variable expression—even family members with the same genetic makeup may show different levels of symptom severity. The gene(s) may express as Tourette syndrome, as a milder tic disorder (transient or chronic tics), or as obsessive compulsive symptoms with no tics at all.[12] Only a minority of the children who inherit the gene(s) will have symptoms severe enough to require medical attention.[13] There is currently no way to predict the symptoms a child may display, even if the gene(s) are inherited.
Recent research suggests that a small number of Tourette syndrome cases may be caused by a defect on chromosome 13 of gene SLITRK1. Some cases of tourettism (tics due to reasons other than inherited Tourette's syndrome) can be caused by mutation.[11] The finding of a chromosomal abnormality appears to apply to a very small minority of cases (1–2%).
Pathophysiology
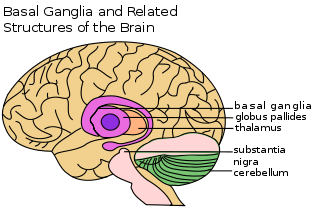
The exact mechanism affecting the inherited vulnerability has not been established, and the precise cause of Tourette syndrome is not known. Tics are believed to result from dysfunction in the central nervous system,[9] in the cortical and subcortical regions, the thalamus, basal ganglia, and frontal cortex of the brain.[3] Neuroanatomic models implicate failures in circuits connecting the brain's cortex and subcortex,[5] and imaging techniques implicate the basal ganglia and frontal cortex.[14][15][16] Research presents considerable evidence that abnormal activity of the brain chemical, or neurotransmitter, dopamine is involved.[17] Dopamine excess or supersensitivity of the postsynaptic dopamine receptors may be an underlying mechanism of Tourette syndrome.[18][19][20][21]
Multiple neurotransmitters, like histamine (H3R), dopamine, serotonin, GABA and glutamate are involved in the etiology.[6] After 2010, the central role of histamine (H3-receptor in the basal ganglia) came into focus in the pathophysiology of Tourette Syndrome.[22] The striatum is the main input nucleus of the basal ganglia circuit in the disorder, which is linked to the involvement of the histaminergic H3-receptor.[23]
Non-genetic influences
Non-genetic, environmental, infectious, or psychosocial factors—while not causing Tourette's—can influence the severity of the disorder.[5] Twin studies have shown that the twin with lower birth weight is more likely to have more noticeable symptoms.[24][25] Other perinatal events, such as maternal stress,[25][26] maternal smoking,[25][27] and obstetric complications,[28] while not causing tics, may be risk factors for increased severity of tics. Most studies of prenatal and perinatal risk factors for tics, TS, or worsening severity of symptoms are of poor quality.[25] Autoimmune processes may affect tic severity in some cases: the unproven and contentious hypothesis that Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal infections, PANDAS, plays a role in the onset of tic disorders and OCD is a current focus of research.[29][30]
Relation with OCD and ADHD
Some forms of obsessive-compulsive disorder (OCD) may be genetically linked to Tourette's, or an alternate expression of the condition;[31] genetic studies show an increased rate of tics and obsessive-compulsive behaviors or OCD in relatives of patients with Tourette's, and "reinforce the idea that at least some forms of OCD are etiologically related to TS, and may, therefore, be a variant expression of the same etiologic factors that are important for the expression of tics."[32] Further evidence supporting that OCD and Tourette's are alternative expressions of a common genetic vulnerability is that males inheriting the genetic vulnerability are more likely to display tics, while females are more likely to display obsessive-compulsive traits.[9]
The genetic relationship of attention-deficit hyperactivity disorder (ADHD) to Tourette's syndrome is less clear, with some evidence to suggest no genetic linkage, and some evidence to suggest that some forms of Tourette's syndrome may be genetically related to ADHD.[33] Not all persons with Tourette's syndrome will have ADHD or OCD, although in specialty clinics where the most impaired patients are treated, a high percentage of patients seeking treatment do have ADHD.[9] The high co-occurrence of ADHD observed in specialty clinics may be due to clinical ascertainment bias. Further study is needed to understand the genetic relationship between ADHD and Tourette's.[33]
Notes
- ↑ American Psychiatric Association (2013). Diagnostic and Statistical Manual of Mental Disorders (Fifth ed.). Arlington, VA: American Psychiatric Publishing. pp. 81–85. ISBN 978-0-89042-555-8.
- ↑ Black, KJ. Tourette Syndrome and Other Tic Disorders. eMedicine (March 22, 2006). Retrieved on June 27, 2006.
- 1 2 3 Walkup JT, Mink JW, Hollenback PJ, (eds). Advances in Neurology, Vol. 99, Tourette Syndrome. Lippincott Williams & Wilkins, Philadelphia, PA, 2006, p. xv. ISBN 0-7817-9970-8
- ↑ Robertson MM. "Tourette syndrome, associated conditions and the complexities of treatment" (PDF). Brain. 2000;123 Pt 3:425–62. doi:10.1093/brain/123.3.425 PMID 10686169
- 1 2 3 4 5 Zinner SH. Tourette disorder. Pediatr Rev. 2000;21(11):372. PMID 11077021
- 1 2 Paschou P, Fernandez TV, Sharp F, Heiman GA, Hoekstra PJ. "Genetic Susceptibility and Neurotransmitters in Tourette Syndrome". International review of neurobiology. 2013;112:155–77. PMID 24295621 doi:10.1016/B978-0-12-411546-0.00006-8
- ↑ Pauls DL. The genetics of Tourette syndrome. Curr Psychiatry Rep. 2001 Apr;3(2):152-7. PMID 11276411
- ↑ Robertson MM. Tourette syndrome, associated conditions and the complexities of treatment. Brain. 2000;123 Pt 3:425–462. p. 425. doi:10.1093/brain/123.3.425 PMID 10686169
- 1 2 3 4 Bagheri MM, Kerbeshian J, Burd L. Recognition and management of Tourette's syndrome and tic disorders. Am Fam Physician. 1999; 59:2263–2274. PMID 10221310 Full text.
- ↑ Freeman, RD. Tourette's Syndrome: minimizing confusion. Retrieved on February 8, 2006.
- 1 2 Mejia NI, Jankovic J. Secondary tics and tourettism. Rev Bras Psiquiatr. 2005;27(1):11-7. PMID 15867978 Full-text PDF
- ↑ van de Wetering BJ, Heutink P. The genetics of the Gilles de la Tourette syndrome: a review. J Lab Clin Med. 1993 May;121(5):638–45. PMID 8478592
- ↑ Tourette Syndrome Association. Tourette Syndrome: Frequently Asked Questions. Retrieved on February 8, 2005.
- ↑ Haber SN, Wolfer D. Basal ganglia peptidergic staining in Tourette syndrome. A follow-up study. Adv Neurol. 1992;58:145-50. PMID 1414617
- ↑ Peterson B, Riddle MA, et al. Reduced basal ganglia volumes in Tourette's syndrome using three-dimensional reconstruction techniques from magnetic resonance images. Neurology. 1993;43:941-9. PMID 8492950
- ↑ Moriarty J, Varma AR, et al. A volumetric MRI study of Gilles de la Tourette's syndrome. Neurology. 1997;49:410-5. PMID 9270569
- ↑ Singer HS, Walkup JT. Tourette syndrome and other tic disorders. Diagnosis, pathophysiology, and treatment. Medicine. 1991;70:15–32. PMID 1988764
- ↑ Singer HS, Butler IJ, et al. Dopaminergic dysfunction in Tourette syndrome. Ann Neurol. 1982;12:361-6. PMID 6184010
- ↑ Klawans HL, Falk DK, Nausieda PA, Weiner WJ. Gilles de la Tourette syndrome after long-term chlorpromazine therapy. Neurology. 1978;28:1064–6. PMID 284201
- ↑ Butler IJ, Koslow SH, et al. Biogenic amine metabolism in Tourette syndrome. Ann Neurol. 1979;6:37-9. PMID 292354
- ↑ Singer HS. Neurobiology of Tourette syndrome. Neurol Clin. 1997;15:357-79. PMID 9115467
- ↑ Rapanelli M, Pittenger C. “Histamine and Histamine Receptors in Tourette Syndrome and Other Neuropsychiatric Conditions”. Neuropharmacology, 2016 Jul;106:85–90. PMID 26282120 doi:10.1016/j.neuropharm.2015.08.019
- ↑ Bolam, J. Paul, and Tommas J. Ellender. “Histamine and the Striatum.” Neuropharmacology, 2016 Jul;106:74–84. PMID 26275849 doi: 10.1016/j.neuropharm.2015.08.013
- ↑ Hyde TM, Aaronson BA, Randolph C, et al. Relationship of birth weight to the phenotypic expression of Gilles de la Tourette's syndrome in monozygotic twins. Neurology. 1992 Mar;42 (3 Pt 1):652-8. PMID 1549232
- 1 2 3 4 Chao TK, Hu J, Pringsheim T. Prenatal risk factors for Tourette Syndrome: a systematic review. BMC Pregnancy Childbirth. 2014 Jan 30;14:53. doi:10.1186/1471-2393-14-53 PMID 24479407
- ↑ Leckman JF, Dolnansky ES, Hardin MT, et al. Perinatal factors in the expression of Tourette's syndrome: an exploratory study. J Am Acad Child Adolesc Psychiatry. 1990 Mar;29(2):220-6. PMID 1969861
- ↑ Mathews CA, Bimson B, Lowe TL, et al. Association between maternal smoking and increased symptom severity in Tourette's syndrome. Am J Psychiatry. 2006 Jun;163(6):1066–73. PMID 16741208
- ↑ Santangelo SL, Pauls DL, Goldstein JM, et al. Tourette's syndrome: what are the influences of gender and comorbid obsessive-compulsive disorder? J Am Acad Child Adolesc Psychiatry. 1994 Jul-Aug;33(6):795–804. PMID 8083136
- ↑ Swerdlow, NR. Tourette Syndrome: Current Controversies and the Battlefield Landscape. Curr Neurol Neurosci Rep. 2005, 5:329–331. doi:10.1007/s11910-005-0054-8 PMID 16131414
- ↑ Kurlan R, Kaplan EL. The pediatric autoimmune neuropsychiatric disorders associated with streptococcal infection (PANDAS) etiology for tics and obsessive-compulsive symptoms: hypothesis or entity? Practical considerations for the clinician. Pediatrics. 2004 Apr;113(4):883-6. doi:10.1542/peds.113.4.883 PMID 15060240
- ↑ Pauls DL, Towbin KE, Leckman JF, et al. Gilles de la Tourette's syndrome and obsessive-compulsive disorder. Evidence supporting a genetic relationship. Arch Gen Psychiatry. 1986 Dec;43(12):1180–2. PMID 3465280
- ↑ Cohen DJ, Jankovic J, Goetz CG, (eds). Advances in Neurology, Vol. 85, Tourette Syndrome. Lippincott, Williams & Wilkins, Philadelphia, PA, 2001.
- 1 2 Leckman JF, Cohen DJ. Tourette's Syndrome—Tics, Obsessions, Compulsions: Developmental Psychopathology and Clinical Care. John Wiley & Sons, Inc., New York, 1999.
External links
- The Genetics of Gilles de la Tourette Syndrome — 53-minute video where David Pauls discusses the results of a genetic linkage study for Tourette syndrome.