Hyphema
Hyphema is a condition that occurs when blood enters the front (anterior) chamber of the eye between the iris and the cornea.[1] People usually first notice a loss of vision or decrease in vision.[1] They eye may also appear to have a reddish tinge, or it may appear as a small pool of blood at the bottom of the iris or in the cornea. A traumatic hyphema is caused by a hit to the eye from a projected object or a blow to the eye.[1] A hyphema can also occur spontaneously.[2]
| Hyphema | |
|---|---|
| Other names | Hyphaema |
 | |
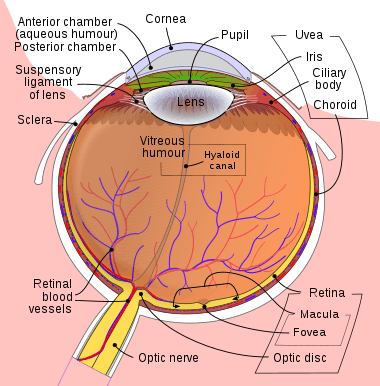
| Hyphema - occupying half of anterior chamber of eye | |
| Specialty | Ophthalmology |
Presentation
A decrease in vision or a loss of vision is often the first sign of a hyphema.[1] People with microhyphema may have slightly blurred or normal vision. A person with a full hyphema may not be able to see at all (complete loss of vision).[1] The person's vision may improve over time as the blood moves by gravity lower in the anterior chamber of the eye, between the iris and the cornea.[1] In many people, the vision will improve, however some people may have other injuries related to trauma to the eye or complications related to the hyphema.[1] A microhyphema, where red blood cells are hanging in the anterior chamber of the eye, is less severe. A layered hyphema when fresh blood is seen lower in the anterior chamber is moderately severe. A full hyphema (total hyphema), when blood fills up the chamber completely, is the most severe.[1]
Complications
While the vast majority of hyphemas resolve on their own without issue, sometimes complications occur.[1] Traumatic hyphema may lead to increased intraocular pressure (IOP), peripheral anterior synechiae, atrophy of the optic nerve, staining of the cornea with blood, re-bleeding, and impaired accommodation.[3]
Secondary hemorrhage, or rebleeding of the hyphema, is thought to worsen outcomes in terms of visual function and lead to complications such as glaucoma, corneal staining, optic atrophy, or vision loss.[1] Rebleeding occurs in 4–35% of hyphema cases and is a risk factor for glaucoma.[4] Young children with traumatic hyphema are at an increased risk of developing amblyopia, an irreversible condition.[1]
Causes
Hyphemas are frequently caused by injury, and may partially or completely block vision. The most common causes of hyphema are intraocular surgery, blunt trauma, and lacerating trauma. Hyphemas may also occur spontaneously, without any inciting trauma. Spontaneous hyphemas are usually caused by the abnormal growth of blood vessels (neovascularization), tumors of the eye (retinoblastoma or iris melanoma), uveitis, or vascular anomalies (juvenile xanthogranuloma).[2] Additional causes of spontaneous hyphema include: rubeosis iridis, myotonic dystrophy, leukemia, hemophilia, and von Willebrand disease.[3] Conditions or medications that cause thinning of the blood, such as aspirin, warfarin, or drinking alcohol may also cause hyphema. Source of bleeding in Hyphema with blunt trauma to eye is Circulus Iridis Major artery.
Treatment

The main goals of treatment are to decrease the risk of re-bleeding within the eye, corneal blood staining, and atrophy of the optic nerve. Small hyphemas can usually be treated on an outpatient basis. There is little evidence that most of the commonly used treatments for hyphaemia (antifibrinolytic agents (oral and systemic aminocaproic acid, tranexamic acid, and aminomethylbenzoic acid), corticosteroids (systemic and topical), cycloplegics, miotics, aspirin, conjugated estrogens, traditional Chinese medicine, monocular versus bilateral patching, elevation of the head, and bed rest) are effective at improving visual acuity after two weeks.[1] Surgery may be necessary for non-resolving hyphemas, or hyphaemas that are associated with high pressure that does not respond to medication. Surgery can be effective for cleaning out the anterior chamber and preventing corneal blood staining.[3]
If pain management is necessary, acetaminophen can be used. Aspirin and ibuprofen should be avoided, because they interfere with platelets' ability to form a clot and consequently increase the risk of additional bleeding.[5] Sedation is not usually necessary for patients with hyphema.
Aminocaproic or tranexamic acids are often prescribed for hyphema on the basis that they reduce the risk of rebleeding by inhibiting the conversion of plasminogen to plasmin, and thereby keeping clots stable.[4] However, the evidence for their effectiveness is limited and amioncaproic acid may actually cause hyphemas to take longer to clear.[1]
Prognosis
Hyphemas require urgent assessment by an optometrist or ophthalmologist as they may result in permanent visual impairment.
A long-standing hyphema may result in hemosiderosis and heterochromia. Blood accumulation may also cause an elevation of the intraocular pressure. On average, the increased pressure in the eye remains for six days before dropping.[2] Most uncomplicated hyphemas resolve within 5–6 days.[2]
Epidemiology
As of 2012, the rate of hyphemas in the United States are about 20 cases per 100,000 people annually.[2] The majority of people with a traumatic hympema are children and young adults.[1] 60% of traumatic hyphemas are sports-related, and there are more cases in males compared to females.[1]
See also
References
- Gharaibeh, Almutez; Savage, Howard I.; Scherer, Roberta W.; Goldberg, Morton F.; Lindsley, Kristina (2019). "Medical interventions for traumatic hyphema". The Cochrane Database of Systematic Reviews. 1: CD005431. doi:10.1002/14651858.CD005431.pub4. ISSN 1469-493X. PMC 6353164. PMID 30640411.
- Sheppard, John D. "Hyphema". WebMD, LLC. Medscape. Retrieved 29 November 2012.
- Walton, William; Von Hagen, Stanley; Grigorian, Ruben; Zarbin, Marco (July–August 2002). "Management of Traumatic Hyphema". Survey of Ophthalmology. 47 (4): 297–334. doi:10.1016/S0039-6257(02)00317-X. PMID 12161209. Retrieved 29 November 2012.
- Recchia, Franco M.; Aaberg Jr., Thomas; Sternberg Jr., Paul (2006-01-01). Hinton, David R.; Schachat, Andrew P.; Wilkinson, C. P. (eds.). Chapter 140 - Trauma: Principles and Techniques of Treatment A2 - Ryan, Stephen J. Edinburgh: Mosby. pp. 2379–2401. doi:10.1016/b978-0-323-02598-0.50146-4. ISBN 9780323025980.
- Crawford, JS; Lewandowski, RL; Chan, W (September 1975). "The effect of aspirin on rebleeding in traumatic hyphema". American Journal of Ophthalmology. 80 (3 Pt 2): 543–5. doi:10.1016/0002-9394(75)90224-X. PMC 1311523. PMID 1163602.
External links
| Classification | |
|---|---|
| External resources |