Cerebral amyloid angiopathy
Cerebral amyloid angiopathy (CAA), is a form of angiopathy in which amyloid beta peptide deposits in the walls of small to medium blood vessels of the central nervous system and meninges.[2][3] The term congophilic is sometimes used because the presence of the abnormal aggregations of amyloid can be demonstrated by microscopic examination of brain tissue after staining with Congo red. The amyloid material is only found in the brain and as such the disease is not related to other forms of amyloidosis.[4]
| Cerebral amyloid angiopathy | |
|---|---|
| Other names | Congophilic angiopathy[1] |
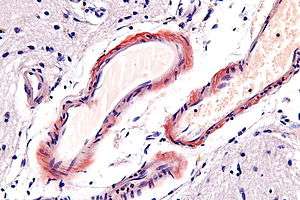 | |
| Micrograph of cerebral amyloid angiopathy using congo red stain | |
| Specialty | Neurology |
| Causes | Cause of CAA is unknown[2] |
| Diagnostic method | PET scan, CT scan[2] |
| Treatment | Management can be physical, occupational, or speech therapy.[2] |
Signs and symptoms
Since this can be caused by the same amyloid protein that is associated with Alzheimer's dementia, brain bleeds[5] are more common in people who have a diagnosis of Alzheimer's disease. However, they can also occur in those who have no history of dementia. The bleeding within the brain is usually confined to a particular lobe[6] and this is slightly different compared to brain bleeds which occur as a consequence of high blood pressure (hypertension) - a more common cause of a hemorrhagic stroke (or bleeding in the brain).[7]
Causes
CAA has been identified as occurring either sporadically (generally in elderly populations)[8] or in familial forms such as Flemish, Iowa, and Dutch types. In all cases, it is defined by the deposition of Aβ in the leptomeningal and cerebral vessel walls.[9] CAA occurring in the Flemish type has been observed to be linked to large dense-core plaques observed in this pedigree.[10]
The reason for increased deposition of Aβ in sporadic CAA is still unclear with both increased production of the peptide and abnormal clearance having been proposed as potential causes.[11] Under normal physiology Aβ is cleared from the brain by four pathways: (1) endocytosis by astrocytes and microglial cells, (2) enzymatic degradation by neprilysin or insulysin (3) cleared by way of the blood brain barrier or (4) drained along periarterial spaces. Abnormalities in each of these identified clearance pathways have been linked to CAA.[12][13]
In familial forms of CAA, the cause of Aβ build up is likely due to increased production rather than poor clearance.[14] Mutations in the amyloid precursor protein (APP), Presenilin (PS) 1 and PS2 genes can result in increased rates of cleavage of the APP into Aβ. An immune mechanism has also been proposed.[15][16] apolipoprotein E (APOE) ε2 and ε4 are associated with increased risk of getting cerebral amyloid antipathy. The use of antiplatelet and anticoagulant therapy increases the risk of getting intracerebral haemorrhage in CAA.[17]
Types
It is usually associated with amyloid beta.[18]
However, there are other types:
- the "Icelandic type" is associated with Cystatin C[19]
- the "British type" is associated with ITM2B[20]
Research is currently being conducted to determine if there is a link between cerebral amyloid angiopathy and ingestion of excessive quantities of aluminium.[21]
Diagnosis
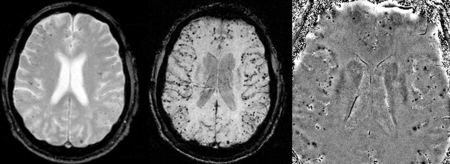
CAA can only be definitively diagnosed by a post-mortem autopsy.[23] Biopsies can play a role in diagnosing probable cases.[24] When no tissue is available for biopsy, the Boston Criteria are used to determine probable CAA cases from MRI or CT scan data. The Boston Criteria require evidence of multiple lobar or cortical hemorrhages to label a patient as probably having CAA.[23] Susceptibility weighted imaging has been proposed as a tool for identifying CAA-related microhemorrhages.[25]
Imaging
Cerebral amyloid angiopathy can be presented with lobar intracerebral hemorrhage or microbleeds in the brain. The bleeding usually occurs on the surfaces of the brain in contrast with intracranial haemorrhage due to high blood pressure which occurs deep locations of the brain such as basal ganglia and pons. In lobar intracerebral bleed, computed tomography (CT) scan would show hyperdense haemorrhage area and hypodense odema around the haemorrhagic site.[17]
MRI sequence of gradient echo and Susceptibility weighted imaging(SWI) are useful in detecting microbleeds and deposition of iron on the brain cortex (cortical superficial siderosis).[17]
Management
The aim in cerebral amyloid angiopathy is to treat the symptoms, as there is no current cure. Physical, occupational and/or speech therapy may be helpful in the management of this condition.[2]
References
- Exley C, Esiri MM (July 2006). "Severe cerebral congophilic angiopathy coincident with increased brain aluminium in a resident of Camelford, Cornwall, UK". J. Neurol. Neurosurg. Psychiatry. 77 (7): 877–9. doi:10.1136/jnnp.2005.086553. PMC 2117501. PMID 16627535.
- "Cerebral amyloid angiopathy: MedlinePlus Medical Encyclopedia". www.nlm.nih.gov. Retrieved 2015-05-27.
- "UpToDate". www.uptodate.com. Retrieved 2019-08-17.
- Newfoundland, FRCP William Pryse-Phillips MD, FRCP(C) Faculty of Medicine Health Sciences Centre Memorial University of Newfoundland St John's (2009-05-06). Companion to Clinical Neurology. Oxford University Press, USA. ISBN 9780199710041.
- Godefroy, Olivier (2013-02-28). The Behavioral and Cognitive Neurology of Stroke. Cambridge University Press. ISBN 9781107310896.
- Coleman, William B.; Tsongalis, Gregory J. (2010-02-16). Essential Concepts in Molecular Pathology. Academic Press. ISBN 9780080922188.
- "Brain Basics: Preventing Stroke: National Institute of Neurological Disorders and Stroke (NINDS)". www.ninds.nih.gov. Retrieved 2015-05-27.
- Sirven, Joseph I.; Malamut, Barbara L. (2008). Clinical Neurology of the Older Adult. Lippincott Williams & Wilkins. ISBN 9780781769471.
- Ettinger, Alan B.; Weisbrot, Deborah M. (2014-04-17). Neurologic Differential Diagnosis: A Case-Based Approach. Cambridge University Press. ISBN 9781107014558.
- Kumar-Singh, S.; Cras, P.; et al. (2002). "Dense-core senile plaques in the Flemish variant of Alzheimer's disease are vasocentric". American Journal of Pathology. 161 (2): 507–20. doi:10.1016/S0002-9440(10)64207-1. PMC 1850756. PMID 12163376.
- Tolnay, Markus; Probst, Alphonse (2012-12-06). Neuropathology and Genetics of Dementia. Springer Science & Business Media. ISBN 9781461512493.
- Subramaniam, Rathan; Barrio, Jorge (2013-10-15). Novel Imaging Techniques in Neurodegenerative and Movement Disorders, an Issue of Pet Clinics. Elsevier Health Sciences. ISBN 9780323227353.
- Brain Extracellular Matrix in Health and Disease. Elsevier. 2014-10-30. ISBN 9780444634948.
- Hall, Tim (2013-09-17). PACES for the MRCP: with 250 Clinical Cases. Elsevier Health Sciences. ISBN 978-0702054662.
- Mental Disorders: New Insights for the Healthcare Professional: 2011 Edition. ScholarlyEditions. 2012-01-09. ISBN 9781464900853.
- Advances in Dementia Research and Treatment: 2012 Edition. ScholarlyEditions. 2012-12-26. ISBN 9781464991721.
- Sharma, Rohit; Dearaugo, Stephanie; Infeld, Bernard; O'Sullivan, Richard; Gerraty, Richard P (August 2018). "Cerebral amyloid angiopathy: Review of clinico-radiological features and mimics". Journal of Medical Imaging and Radiation Oncology. 62 (4): 451–463. doi:10.1111/1754-9485.12726.
- Dickson, Dennis; Weller, Roy O. (2011-09-09). Neurodegeneration: The Molecular Pathology of Dementia and Movement Disorders. John Wiley & Sons. ISBN 9781444341232.
- Larner, A. J. (2008-04-24). Neuropsychological Neurology: The Neurocognitive Impairments of Neurological Disorders. Cambridge University Press. ISBN 9780521717922.
- Dening, Tom; Thomas, Alan (2013-09-26). Oxford Textbook of Old Age Psychiatry. OUP Oxford. ISBN 9780199644957.
- Kawahara, Masahiro; Kato-Negishi, Midori (2011). "Link between Aluminum and the Pathogenesis of Alzheimer's Disease: The Integration of the Aluminum and Amyloid Cascade Hypotheses". International Journal of Alzheimer's Disease. 2011: 276393. doi:10.4061/2011/276393. ISSN 2090-0252. PMC 3056430. PMID 21423554.
- Mittal, S.; Wu, Z.; Neelavalli, J.; Haacke, E. M. (2009). "Susceptibility-Weighted Imaging: Technical Aspects and Clinical Applications, Part 2". American Journal of Neuroradiology. 30 (2): 232–252. doi:10.3174/ajnr.A1461. ISSN 0195-6108. PMC 3805373. PMID 19131406.
- Greenberg, Steven; Charidimou, Andreas (2018). "Diagnosis of Cerebral Amyloid Angiopathy: Evolution of the Boston Criteria". Stroke. 49 (2): 491–497. doi:10.1161/STROKEAHA.117.016990. PMC 5892842. PMID 29335334.
- Verbeek, M. M.; Waal, R. M. de; Vinters, Harry V. (2013). Cerebral Amyloid Angiopathy in Alzheimer's Disease and Related Disorders. Springer Science & Business Media. ISBN 9789401710077.
- Ellenbogen, Richard G.; Abdulrauf, Saleem I.; Sekhar, Laligam N. (2012). Principles of Neurological Surgery. Elsevier Health Sciences. ISBN 978-1437707014.
Further reading
- Chao, Christine P.; Kotsenas, Amy L.; Broderick, Daniel F. (September 1, 2006). "Cerebral Amyloid Angiopathy: CT and MR Imaging Findings". RadioGraphics. 26 (5): 1517–1531. doi:10.1148/rg.265055090. ISSN 0271-5333. PMID 16973779.
External links
| Classification | |
|---|---|
| External resources |