Buruli ulcer
Buruli ulcer is an infectious disease characterized by the development of painless open wounds, most commonly on the limbs.[2] The first sign of infection is often a small painless nodule or area of swelling. Over days to weeks, this nodule can grow larger under the skin. Eventually surface skin sloughs off the expanding wound, causing an open ulcer. Deep ulcers can cause scarring of muscles and tendons, resulting in permanent disability. Buruli ulcer most commonly affects the arms or legs, but can occur anywhere on the body.[3]
| Buruli ulcer | |
|---|---|
| Other names | Bairnsdale ulcer, Bairnsdale ulcer, Daintree ulcer, Mossman ulcer, Kumasi ulcer, Sears ulcer[1] |
 | |
| Buruli ulcer on the ankle of a person from Ghana. | |
| Specialty | Infectious disease |
| Symptoms | Area of swelling that becomes an ulcer[2] |
| Causes | Mycobacterium ulcerans[2] |
| Treatment | Rifampicin and streptomycin[2] |
| Frequency | at least 2000 to 5000 cases per year[2] |
Buruli ulcer is caused by skin infection with Mycobacterium ulcerans. Bacteria live in aquatic environments, particularly in slow-moving or stagnant water, from which they are somehow introduced to humans. The mechanism by which M. ulcerans is transmitted from the environment to humans is not known; however, M. ulcerans cannot be transmitted from one human to another.[1] Once in the skin M. ulcerans grows and releases the toxin mycolactone which blocks the normal function of cells, resulting in tissue death and immune suppression.
The World Health Organization recommends treating Buruli ulcer with a combination of the antibiotics rifampicin and streptomycin, administered daily for 8 weeks.[4] Due to inconvenience of taking streptomycin, which must be injected daily by a healthcare provider, several all-oral antibiotic combinations are being tried across the world. For severe ulcers, treatment may include surgery to remove dead tissue or repair scarred muscles or joints. Healthy skin may be grafted onto larger ulcers to promote healing. Even treated ulcers can take weeks or months to heal; regular wound cleaning and dressing is done to aid healing and prevent infection.
About 2,000 cases are reported a year.[5] Buruli ulcers occur most commonly in rural sub-Saharan Africa and Australia with fewer cases in South America and the Western Pacific.[5] Children are most commonly infected in Africa, while adults are most commonly affected in Australia.[5] Cases have been reported in 33 countries.[5] The disease also occurs in animals other than humans, though no link between animal and human infection has been established.[6] Albert Ruskin Cook was the first to describe buruli ulcers in 1897.[7] It is classified as a neglected tropical disease.[8]
Signs and symptoms
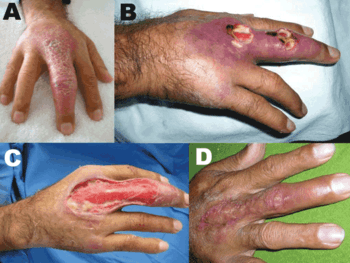
The first sign of Buruli is the appearance of a painless swollen area on the arm or leg. This most commonly takes the form of a small bump, similar in appearance to an insect bite.[9][2] However, sometimes the first sign is a patch of firm, raised skin about three centimeters across called a "plaque"; or a more widespread swelling under the skin.[9][2] Over the course of a few weeks, the original swollen area may expand, forming an irregularly shaped patch of swollen skin.[9][3] After about four weeks, the affected skin sloughs off, leaving a large painless ulcer.[2] In some people, the ulcer remains small and may linger unhealed for years.[3] In others, the ulcer continues to grow wider and sometimes deeper, with skin at the margin dying and sloughing off, and underlying muscle, tendon, and bone sometimes exposed.[3] Ulcers can extend into muscles and tendons, causing parts of these tissues to be replaced by inelastic scar tissue, immobilizing the body part and resulting in permanent disability.[3] Large exposed ulcers are often infected by other bacteria, causing the wound to smell foul.[3]
Buruli ulcers can appear anywhere on the body, but are far more common on the limbs than elsewhere. Ulcers are most common on the lower limbs (62%) and upper limbs (24%), but can also be found on the trunk (9%), head/neck (3%), or genitals (less than 1%).[10] The World Health Organization classifies Buruli ulcer cases into three categories depending on the severity of their symptoms. A single small (less than five centimeters) ulcer is category I. Larger ulcers (up to 15 centimeters) are category II. Ulcers that are larger, disseminated across the body, or include particularly sensitive sites (e.g. the eyes, bones, joints, or genitals) are called category III.[3]
Cause
Buruli ulcer is caused by infection of the skin with the bacterium Mycobacterium ulcerans.[2] M. ulcerans infections typically occur near slow-moving or stagnant bodies of water, where M. ulcerans can be found in aquatic insects, mollusks, fish, and the water itself.[1] How M. ulcerans is transmitted to humans remains unclear, but somehow bacteria enter the skin and begin to grow. Disease is primarily caused by a toxin produced by the bacteria, mycolactone.[11] As the bacteria grow, they release mycolactone, which diffuses into host cells and blocks the action of Sec61, the core translocation protein that serves as the gateway to the endoplasmic reticulum.[12] When Sec61 is blocked, proteins that would normally enter the endoplasmic reticulum are instead translated into the cytosol, causing a pathological stress response that results in cell death by apoptosis.[12] This results in large-scale tissue death at the site of infection, causing the large open ulcer characteristic of disease.[12] At the same time, Sec61 inhibition prevents cells from signalling to activate the immune system, resulting in ulcers that lack infiltrating immune cells.[12]
Transmission

It is not known how M. ulcerans is introduced to humans.[2] Human-to-human transmission is extremely rare, and Buruli ulcer is not considered contagious.[1] In areas endemic for Buruli ulcer, cases tend to be found near stagnant bodies of water, leading to the long-standing hypothesis that M. ulcerans is somehow transmitted to humans from aquatic environments.[13] Supporting this model, M. ulcerans is widespread in aquatic environments, where it can survive as free-living or associated with other aquatic organisms.[10] Live M. ulcerans has been isolated from aquatic insects, mosses, and animal feces; and its DNA has been found in water, soil, mats of bacteria and algae, fish, crayfish, aquatic insects, and other animals that live in or near water.[13] A role for biting insects in transmission has long been investigated, with particular focus on mosquitoes, giant water bugs, and Naucoridae. M. ulcerans is occasionally found in these insects, and they can sometimes transmit the bacteria in certain laboratory settings.[10] However, whether these insects are regularly involved in transmission remains unclear.[1][13] Pre-existing wounds have also been implicated in disease transmission, and poor wound care is associated with a higher risk of acquiring Buruli ulcer.[14] Consistent with this, wearing long pants and long-sleeved shirts is associated with a lower risk of Buruli ulcer, possibly by preventing insect bites or protecting wounds.[1][14]
Genetic susceptibility
While Buruli ulcer is not contagious, susceptibility sometimes runs in families, suggesting genetics could play a role in who develops disease. Severe Buruli ulcer in a Beninese family was attributed to a loss of 37 kilobases of chromosome 8 in a region that included a long non-coding RNA and was near the genes for beta-defensins.[15][16] Additionally, genome-wide association studies have linked susceptibility to Buruli ulcer to variations in six genes: SLC11A1, PRKN, NOD2, ATG16L1, iNOS, and IFNG, as well as in two long non-coding RNAs.[15]
Diagnosis
As most cases of Buruli ulcer arise in low-resource settings, treatment for Buruli ulcer is often initiated by a clinician based on the signs and symptoms alone.[17] Diagnosis is then confirmed by microscopy to detect mycobacteria or PCR to detect M. ulcerans DNA.[18] For microscopy, ulcer material is typically taken by fine-needle aspiration or swabbing the edge of the ulcer, then stained with the Ziehl-Neelsen stain which makes mycobacteria easy to see.[18] However, in practice this method detects just 30-40% of cases, making it a relatively insensitive diagnostic test.[19] The current gold standard test is real-time PCR to detect a sequence termed IS2404 that is unique to M. ulcerans.[20] This method detects 54-84% of cases, and is highly specific to M. ulcerans.[19] However, the equipment required to run real-time PCR is prohibitively expensive, and often available only at centralized diagnostic laboratories; consequently, PCR may be used to confirm a diagnosis well after treatment has begun, rather than to guide initial treatment decisions.[17]
For many bacterial infections, the gold standard for diagnosis is isolating and growing the infective organism in laboratory media. M. ulcerans can be grown in laboratory media, but its extremely slow growth rate prevents this from being used diagnostically; even under optimal growth conditions, the bacteria must grow for 9 to 12 weeks before they can be easily detected and identified.[19] An additional method of diagnosis is microscopic examination of ulcer tissue by a trained pathologist. However, this requires more invasive sampling of ulcer tissue, as well as specifically trained personnel, and so is rarely used in places where Buruli ulcer is endemic.[21]
Treatment

Buruli ulcer is treated through a combination of antibiotics to kill the bacteria, and wound care or surgery to support the healing of the ulcer. Since 2004, the World Health Organization has recommended 8 weeks of daily treatment with oral rifampicin and intramuscular streptomycin.[4] However, due to the nephrotoxicity of streptomycin, and the inconvenience of daily injections, several other antibiotics to partner with rifampicin have been investigated. The most widely used alternative is rifampicin plus twice daily oral clarithromycin, which is now also recommended by the World Health Organization.[4][22] Several other antibiotics are sometimes used to partner with rifampicin, namely ciprofloxacin, moxifloxacin, ethambutol, amikacin, azithromycin, and levofloxacin.[4] A 2018 Cochrane review suggested that the many antibiotic combinations currently being used are effective treatments, but there is insufficient evidence to determine if any combination is more effective than the others.[23] Approximately 1 in 5 people with Buruli ulcer experience a temporary worsening of symptoms 3 to 12 weeks after they begin taking antibiotics.[24] This syndrome, called a paradoxical reaction, is more common in those with larger ulcers and ulcers on the trunk, and is more common in adults than children.[24] The paradoxical reaction in Buruli ulcer is thought to be due to the immune system responding to the wound as bacteria die and the immune-suppresing mycolactone dissipates.[24]
Treatment may also include surgery to remove necrotic ulcer tissue as well as scar tissue that can deform the muscles and joints.[24] As ulcers can take months to heal, regular wound care plays a major role in treatment.[4] The healing of severe ulcers can sometimes require skin grafts and/or daily wound dressings.[24]
Prevention
Buruli ulcer can be prevented by avoiding contact with aquatic environments in endemic areas; however, for those living in endemic areas, this may not be possible.[4] The risk of acquiring Buruli ulcer can be reduced by wearing long sleeves and pants, using insect repellent, and cleaning and covering any wounds as soon as they're noticed.[24] While there is no specific vaccine for Buruli ulcer, vaccination with the BCG vaccine offers temporary protection from disease.[24][25]
Epidemiology
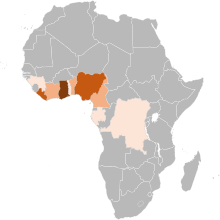
Buruli ulcer is relatively rare, with just 2000-5000 cases reported to the World Health Organization each year.[2] The overwhelming majority of cases are reported from countries in southern West Africa, namely Benin, Côte d'Ivoire, Cameroon, Gabon, Ghana, Guinea, Liberia, Nigeria, and Togo.[26][27] Cases are also regularly reported from southeastern Australia, and more rarely from Papua New Guinea and Japan.[28] Most countries do not report data on Buruli ulcer to the World Health Organization, and the extent of Buruli ulcer's spread is unknown.[29] A 2019 systematic review of existing Buruli ulcer prevalence studies found a clear consensus that Buruli ulcer is present in 12 countries: Australia, Japan, Benin, Côte d'Ivoire, Cameroon, Democratic Republic of Congo, Gabon, Ghana, Liberia, Nigeria, Togo, and South Sudan, as well as "strong" or "very strong" evidence that Buruli ulcer is present in seven additional countries: Republic of Congo, Sierra Leone, Central African Republic, Papua New Guinea, Guinea, Uganda, and French Guiana.[30] Even in countries that do report Buruli ulcer, health systems likely do not record each case due to insufficient reach and resources, and so the reported case numbers are likely underestimates of the true disease prevalence.[31]
Within affected countries, Buruli ulcer cases tend to occur in rural areas near slow-moving or stagnant water.[1] In particular, cases tend to appear near water that has experienced human intervention, such as the building of dams or irrigation systems, flooding, or deforestation.[1] Within endemic communities, few characteristics predict who will acquire Buruli ulcer. Males and females are equally likely to be infected.[1] Ulcers can appear in people of all ages, although infections are most common among children between 5 and 15 years in West Africa, and adults over 40 in Australia and Japan.[32]
History
While M. ulcerans may have infected humans throughout history, the first written description of Buruli ulcer is credited to a British missionary doctor, Albert R. Cook.[33][34] In 1897, at Mengo Hospital in Uganda, Cook noted several patients with slow-healing ulcers, consistent with Buruli ulcer.[35][36] The cause of these slow-healing ulcers was identified 50 years later in 1948, when Peter MacCallum, Jean Tolhurst, Glen Buckle, and H. A. Sissons at Melbourne University described a series of cases from Bairnsdale, Victoria, isolated the causative mycobacterium, and showed it could cause ulcers in laboratory rats.[1][37] Over the following decades, more cases were described in Africa, including a particularly high prevalence in Uganda's Buruli County, leading to the disease becoming more widely known as "Buruli ulcer".[35] In 1998, the World Health Organization started the Global Buruli Ulcer Initiative with the aim of coordinating global efforts to control Buruli ulcer.[35] This was followed in 2004 by World Health Organization Resolution WHA57.1 calling upon member countries to support the Global Buruli Ulcer Initiative and increase research on Buruli ulcer diagnostics and treatment.[38][39]
Other names
Buruli ulcer is known by several other names in different parts of the world. In southeastern Australia, it was originally called "Searls' ulcer" after the physician J. R. Searls who saw the first Australian cases at the Bairnsdale Clinic and sent material to Peter MacCallum's group at Melbourne University for further examination.[40] In subsequent years, the disease became more generally known as "Bairnsdale ulcer" after the district where those cases were described.[35] In northeastern Australia, north of Cairns, the disease is called "Daintree ulcer" or "Mossman ulcer" after the nearby Daintree River and the town of Mossman.[41][42] In Papua New Guinea, the disease is called "Kumusi ulcer" after the Kumusi River along which villages with cases of the disease were originally described.[43]
Research
Buruli ulcer has been the subject of scientific research since the description of M. ulcerans in 1948, and the demonstration that the bacteria could cause ulcers in laboratory animals.[1][37] While several animals are susceptible to M. ulcerans ulcers, mice (particularly BALB/c and C57BL/6 mice) are most commonly used to model Buruli ulcer in modern laboratories.[44] Since M. ulcerans can only grow in relatively cool temperatures, mice are typically infected in furless parts of the body: the ear, tail, or footpad.[44] After injection into the mouse, bacteria double every 3 to 4 days, and the first signs of skin disease appear after 3 to 4 weeks.[45] Strains of M. ulcerans used in laboratores are less standardized than their murine hosts, with different laboratories using different strains based on convenience and accessibility.[46] Three M. ulcerans strains are particularly common: "Cu001", isolated from a person in Adzopé, Côte d'Ivoire in 1996; "Mu1615", from a person in Malaysia in the 1960s; and "S1013" from someone in Cameroon in 2010.[46] Most Buruli ulcer research is focused on testing new antibiotics against the bacteria, testing vaccine candidates, and better understanding how M. ulcerans infection causes disease.[47]
References
- Guarner (2018), pp. 1-2
- "Buruli ulcer (Mycobacterium ulcerans infection)". World Health Organization. 21 May 2019.
- Guarner (2018), pp. 3-4
- Yotsu, et al. (2018) pp. 251-252
- "Buruli ulcer (Mycobacterium ulcerans infection) Fact sheet N°199". World Health Organization. April 2018. Retrieved 17 April 2018.
- "Buruli Ulcer: Transmission". Centers for Disease Control and Prevention. 26 January 2015. Retrieved 17 April 2018.
- Nakanaga, K; Yotsu, RR; Hoshino, Y; Suzuki, K; Makino, M; Ishii, N (2013). "Buruli ulcer and mycolactone-producing mycobacteria". Japanese Journal of Infectious Diseases. 66 (2): 83–8. doi:10.7883/yoken.66.83. PMID 23514902.
- "Neglected Tropical Diseases". cdc.gov. June 6, 2011. Archived from the original on 4 December 2014. Retrieved 28 November 2014.
- Yotsu, et al. (2015) p. 1034
- Zingue, et al. (2018) pp. 10-13
- Yotsu, et al. (2018), pp. 247-8
- Yotsu, et al. (2018), p. 251
- Yotsu, et al. (2018) p. 250
- Jacobsen and Padgett (2010) pp.e678-e679
- Manry (2020) p. 3
- Quentin, et al. (2018) p. e0006429
- Röltgen, et al. (2019) pp. 190-191
- Röltgen, et al. (2019) pp. 185-186
- Guarner (2018) pp. 4-6
- Röltgen, et al. (2019) pp. 186-187
- Röltgen, et al. (2019) pp. 189-190
- "Buruli ulcer (Mycobacterium ulcerans infection) - Treatment". World Health Organization. Retrieved 19 June 2020.
- Yotsu, Richardson, and Ishii (2018) p. 3
- Guarner, et al. (2018) pp. 6-7
- Zimmerman, et al. (2018) pp. 682-684
- "Buruli ulcer - Number of new reported cases - Data by country". World Health Organization. Retrieved 3 June 2020.
- Zingue, et al. (2018) p. 4
- Yotsu, et al. (2018) pp. 248-249
- Simpson, et al. (2019) pp. e912-e913
- Simpson, et al. (2019) pp. e917-e918
- Zingue et al. (2018) pp. 30-31
- Yotsu, et al. (2015) pp. 1033-1034
- Zigue, et al. (2018) pp. 4-8
- van der Werf, et al. (2005) p. 2
- Röltgen K and Pluschke G (2019) pp. 1-2
- "Mengo Hospital medical notes - 1897". British Library. 2017. Retrieved 5 June 2020.
- MacCallum, et al. (1948) pp. 95-98, 103, 117-118
- World Health Organization (2010) p. 62
- World Health Organization (2004) pp. 1-2
- Meyers (2007) p. 1
- O'Brien, et al. (2014) p. 267
- Johsnon (2019) p. 64
- Igo and Murthy (1988) p. 391
- Bolz and Ruf (2019) p. 160-161
- Bolz and Ruf (2019) pp. 163-165
- Bolz and Ruf (2019) pp. 162-163
- Bolz and Ruf (2019) pp. 165-168
Works cited
- Bolz M, Ruf MT (April 2019). "Buruli ulcer in animals and experimental infection models". In Pluschke G, Röltgen K (eds.). Buruli ulcer: Mycobacterium ulcerans disease. Cham, Switzerland: Springer. pp. 159–181.
- Guarner J (April 2018). "Buruli Ulcer: Review of a Neglected Skin Mycobacterial Disease". Journal of Clinical Microbiology. 56 (4): e01507-17. doi:10.1128/JCM.01507-17. PMC 5869816.
- Hausmann-Muela S, Sevcsik A (2019). "Transdisciplinary research and action to stop Buruli ulcer: a case study from philanthropy". In Pluschke G, Röltgen K (eds.). Buruli Ulcer: Mycobacterium Ulcerans Disease. Cham, Switzerland: Springer. pp. 273–287. ISBN 978-3-030-11114-4.
- Igo JD, Murthy DP (1988). "Mycobacterium ulcerans infections in Papua New Guinea: Correlation of clinical, histological, and microbiologic features". American Journal of Tropical Medicine and Hygiene. 38 (2): 391–392. doi:10.4269/ajtmh.1988.38.391.
- Jacobsen KH, Padgett JJ (August 2010). "Risk factors for Mycobacterium ulcerans infection". International Journal of Infectious Diseases. 14 (8): e677–e681. doi:10.1016/j.ijid.2009.11.013.
- Johnson PD (April 2019). "Buruli ulcer in Australia". In Pluschke G, Röltgen K (eds.). Buruli ulcer: Mycobacterium ulcerans disease. Cham, Switzerland: Springer. pp. 61–76.
- MacCallum P, Tolhurst JC, Buckle G, Sissons HA (January 1948). "A new mycobacterial infection in man". Journal of Pathology and Bacteriology. 60: 93–122. doi:10.1002/path.1700600111.
- Manry J (April 2020). "Human genetics of Buruli ulcer". Human Genetics. doi:10.1007/s00439-020-02163-1.
- Meyers DH (July 2007). "Mycobacterium ulcerans infection: an eponymous ulcer". Medical Journal of Australia. 187 (1). doi:10.5694/j.1326-5377.2007.tb01136.x.
- O'Brien D, Jenkin G, Buntine J, Steffen CM, McDonald A, Horne S, Friedman ND, Athan E, Huges A, Callan PP, Johnson PD (March 2014). "Treatment and prevention of Mycobacterium ulcernas infection (Buruli ulcer) in Australia: guideline update". The Medical Journal of Australia. 200 (5): 267–270. doi:10.5694/mja13.11331.
- Röltgen K, Cruz I, Ndung'u JM, Pluschke G (2019). "Laboratory Diagnosis of Buruli Ulcer: Challenges and Future Perspectives". In Pluschke G, Röltgen K (eds.). Buruli Ulcer: Mycobacterium Ulcerans Disease. Cham, Switzerland: Springer. pp. 183–202. ISBN 978-3-030-11114-4.
- Röltgen K, Pluschke G (2019). "Buruli ulcer: history and disease". In Pluschke G, Röltgen K (eds.). Buruli Ulcer: Mycobacterium Ulcerans Disease. Cham, Switzerland: Springer. pp. 1–41. ISBN 978-3-030-11114-4.
- Simpson H, Deribe K, Tabah EN, Peters A, Maman I, Frimpong M, Ampadu E, Phillips R, Sanderson P, Pullan RL, Cano J (July 2019). "Mapping the global distribution of Buruli ulcer: a systematic review with evidence consensus". Lancet Global Health. 7: e912–e922. doi:10.1016/S2214-109X(19)30171-8.
- Vincent QB, Belkadi A, Fayard C, Marion E, Adeye A, Ardant MF, et al. (April 2018). "Microdeletion on chromosome 8p23.1 in a familial form of severe Buruli ulcer". PLoS Neglected Tropical Diseases. 12 (4): e0006429. doi:10.1371/journal.pntd.0006429.
- van der Werf TS, Stienstra Y, Johnson RC, Phillips R, Adjei O, Fleischer B, Wansbrough-Jones MW, Johnson PD, Portaels F, van der Graaf WT, Asiedu K (October 2005). "Mycobacterium ulcerans disease". Bulletin of the World Health Organization. 83 (10): 785–791. PMC 2626418.
- "WHA57.1 - Surveillance and control of Mycobacterium ulcerans disease (Buruli ulcer)" (PDF). World Health Organization. May 2004. Retrieved 14 June 2020.
- Working to overcome the global impact of neglected tropical diseases: First WHO report on neglected tropical diseases. World Health Organization. 2010. ISBN 9789241564090. Retrieved 14 June 2020.
- Yotsu RR, Murase C, Sugawara M, Suzuki K, Nakanaga K, Ishii N, Asiedu K (September 2015). "Revisiting Buruli Ulcer". The Journal of Dermatology. 42 (11): 1033–41. doi:10.1111/1346-8138.13049.
- Yotsu RR, Suzuki K, Simmonds RE, Bedimo R, Ablordey A, Yeboah-Manu D, Phillips R, Asiedu K (September 2018). "Buruli Ulcer: a Review of the Current Knowledge". Current Tropical Medicine Reports. 5 (4): 247–256. doi:10.1007/s40475-018-0166-2. PMC 6223704.
- Yotsu RR, Richardson M, Ishii M (August 2018). "Drugs for treating Buruli ulcer (Mycobacterium ulcerans disease)". Cochrane Database of Systematic Reviews. 8 (8): CD012118. doi:10.1002/14651858.CD012118.pub2. PMC 6513118.
- Zimmerman P, Finn A, Curtis N (July 2018). "Does BCG vaccination protect against nontuberculous mycobacterial infection? A systematic review and meta-analysis". Journal of Infectious Disease. 218 (5): 679–687. doi:10.1093/infdis/jiy207.
- Zingue D, Bouam A, Tian RB, Drancourt M (January 2018). "Buruli Ulcer, a Prototype for Ecosystem-Related Infection, Caused by Mycobacterium ulcerans". Clinical Microbiology Reviews. 31 (1): e0004-17. doi:10.1128/CMR.00045-17. PMC 5740976.
External links
| Classification | |
|---|---|
| External resources |