Abdominoperineal resection
An abdominoperineal resection, formally known as abdominoperineal resection of the rectum and abdominoperineal excision of the rectum is a surgery for rectal cancer or anal cancer. It is frequently abbreviated as AP resection, APR and APER.
| Abdominoperineal resection | |
|---|---|
| Other names | abdominoperineal excision, or Miles operation |
| Specialty | General surgery |
Indication and description
The principal indication for AP resection is a rectal carcinoma situated in the distal (lower) one-third of the rectum.[1] Other indications include recurrent or residual anal carcinoma (squamous cell carcinoma) following initial, usually definitive combination chemoradiotherapy.
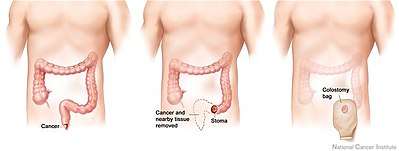
APRs involves removal of the anus, the rectum and part of the sigmoid colon along with the associated (regional) lymph nodes, through incisions made in the abdomen and perineum. The end of the remaining sigmoid colon is brought out permanently as an opening, called a colostomy, on the surface of the abdomen.
Centralisation of rectal surgery
This operation is one of the less commonly performed by general surgeons, although they are specifically trained to perform this operation. As low case volumes in rectal surgery have been found to be associated with higher complication rates,[2][3] it is often centralised in larger centres,[4] where case volumes are higher.
Laparoscopic approach
There are several advantages in terms of outcomes if the surgery can be performed laparoscopically[5]
Relation to low anterior resection (LAR)
An APR, generally, results in a worse quality of life than the less invasive lower anterior resection (LAR).[6][7] Thus, LARs are generally the preferred treatment for rectal cancer insofar as this is surgically feasible.
Eponym
It is named for William Ernest Miles (1869–1947), an English surgeon who published his technique in a landmark paper in 1908.[8]
See also
References
- American Cancer Society. Detailed Guide: Colon and Rectum Cancer. cancer.org. URL: http://www.cancer.org/docroot/CRI/content/CRI_2_4_4x_Surgery_10.asp?sitearea= Archived May 7, 2008, at the Wayback Machine. Accessed on: February 5, 2008.
- Schrag D, Panageas KS, Riedel E, et al. (November 2002). "Hospital and surgeon procedure volume as predictors of outcome following rectal cancer resection". Ann. Surg. 236 (5): 583–92. doi:10.1097/00000658-200211000-00008. PMC 1422616. PMID 12409664.
- Marusch F, Koch A, Schmidt U, Pross M, Gastinger I, Lippert H (October 2001). "Hospital caseload and the results achieved in patients with rectal cancer". Br J Surg. 88 (10): 1397–402. doi:10.1046/j.0007-1323.2001.01873.x. PMID 11578299.
- Martling A, Holm T, Cedermark B (2005). "[Skills by training. Education and case volume are strong prognostic factors in rectal cancer surgery]". Lakartidningen (in Swedish). 102 (6): 374–6. PMID 15754678.
- Simorov A, Reynoso JF, Dolghi Thompson JS, Oleynikov D (2011). "Comparison of perioperative outcomes in patients undergoing laparoscopic versus open abdominoperineal resection". Am J Surg. 202 (6): 666–70. doi:10.1016/j.amjsurg.2011.06.029. PMID 21983001.
- McLeod RS (2001). "Comparison of quality of life in patients undergoing abdominoperineal extirpation or anterior resection for rectal cancer". Ann. Surg. 233 (2): 157–8. doi:10.1097/00000658-200102000-00002. PMC 1421195. PMID 11176119.
- Grumann MM, Noack EM, Hoffmann IA, Schlag PM (2001). "Comparison of quality of life in patients undergoing abdominoperineal extirpation or anterior resection for rectal cancer". Ann. Surg. 233 (2): 149–56. doi:10.1097/00000658-200102000-00001. PMC 1421194. PMID 11176118.
- http://www.whonamedit.com/doctor.cfm/3130.html https://acsjournals.onlinelibrary.wiley.com/doi/abs/10.3322/canjclin.21.6.361?sid=nlm%3Apubmed