Female genital mutilation in the United States
Female genital mutilation (FGM), also known as female circumcision or female genital cutting, includes any procedure involving the removal or injury of part or all of external female genitalia for non medical reasons.[1] While the practice is most common in Africa, Asia, and the Middle East, FGM is also widespread in immigrant communities and metropolitan areas in the United States, and was performed by doctors regularly until the 1980s.[2][3][4]
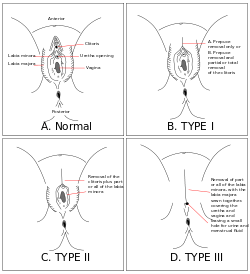
There are four main types of FGM, distinguished by the World Health Organization by their severity.[5] Clitoridectomy, type 1, describes the partial or total removal of the clitoris, and includes circumcision, removal of just the clitoral hood, and clitoridectomy, or removal of the entire clitoral glans and hood.[5][1] Type 2, excision, involves the partial or total removal of the clitoris and labia minora, with or without the additional removal of the labia majora.[1][5] Type 3, infibulation, is the most severe type of FGM. It describes the narrowing of the vaginal opening through creation of a seal, by cutting and repositioning the labia minora or labia majora.[1][5] Type 4 describes any other type of harmful non-medical procedures performed on female genitalia, including cutting, burning, and scraping.[5]
In the United States, FGM is most common in immigrant communities and in major metropolitan areas. Data on the prevalence of FGM in the United States was first collected in 1990, using census information.[6] CDC reports using information from the early 2010-2013 have shown a decrease in FGM in the United States, although growing levels of immigration cause numbers to appear higher.[7]
In addition to its prevalence in immigrant communities in the US, FGM was considered a standard medical procedure in America for most of the 19th and 20th centuries.[8] Physicians performed surgeries of varying invasiveness to treat a number of diagnoses, including hysteria, depression, nymphomania, and frigidity. The medicalization of FGM in the United States allowed these practices to continue until the end of the 20th century, with some procedures covered by Blue Cross Blue Shield Insurance until 1977.[9][8]
With the passage of the Female Genital Mutilation Act in 1996, performing FGM on anyone under age 18 became a felony in the United States.[10] In addition to federal policy, 26 states have made specific laws that prohibit FGM as of 2017.[11] The US has also participated in several UN resolutions that advocate for the eradication of FGM, including the UN's 1948 Universal Declaration of Human Rights, 1989 Convention on the Rights of the Child, and the Convention on the Elimination of All Forms of Discrimination Against Women (CEDAW).[12][3][13]
Prevalence
The current prevalence of FGM in the US is uncertain. In early 2014, Equality Now campaigned with survivor and activist Jaha Dukureh, Representatives Joseph Crowley (D-NY) and Sheila Jackson Lee (D-TX), and The Guardian to petition the Obama Administration to conduct a new prevalence study into the current state of FGM in the U.S. as the first step towards its elimination.[14]
In 1996, the first report on FGM in the United States was developed using data from the 1990 census.[6] It reported that 168,000 girls and women were at risk, with 48,000 under 18.[7] In 2004, the African Women's Health Center at Brigham and Women's Hospital and the PRC revamped these numbers with information from recent surveys and the 2000 U.S. census.[7] They reported 227,887 girls and women at risk in United States, with 62,519 under 18. This increase can be attributed to increases in total immigration.[7]
In 2016, the Centers for Disease Control and Prevention (CDC) released a report compiled with data from 2010-2013. The CDC report estimated 513,000 girls and women in the United States were either victims of FGM or at risk of FGM, with ⅓ under age 18.[15] The marked increase in the number of girls and women at risk of FGM in the United States was attributed to an increase in the total number of immigrants from countries where FGM is most common, not an increase in the frequency of the practice.[16] Of the women at risk, 60% are from 8 states: California, Maryland, Minnesota, New Jersey, New York, Texas, Virginia, and Washington. Additionally, 40% of those reported are concentrated in 5 major metropolitan areas: New York, Washington, Minneapolis-St. Paul, Los Angeles, and Seattle. 55% of the women are from Egypt, Somalia, or Ethiopia.[7] These three "sending countries" have a high prevalence of FGM as well as high numbers of U.S. immigrants.[7] The report used information from US census reports and the American Community Survey (2012) to identify the number of immigrants from countries where FGM is most prevalent.[7]
History
Medicalization
During the 19th century, FGM was frequently performed by doctors as a treatment for many sexual and psychological conditions. During the 19th and 20th centuries, the clitoris was considered the center of female sexuality.[4] In addition, Victorian concepts of female sexuality resulted in a widely-held belief that women were less sexual than men.[17] Female sexuality was typically thought of only within the constructs of heterosexual marriage, and behaviors that strayed from this schema, such as masturbation, were deemed symptomatic, and often resulted in operation on the clitoris.[18][4]
Depending on the symptoms and diagnosis, physicians performed four different procedures of varying invasiveness on women.[4] Doctors would either remove the smegma surrounding the clitoris, lacerate adhesions restricting the clitoris, or remove the clitoral hood altogether (female circumcision).[4] In the most extreme cases, doctors would perform a clitoridectomy, removing the clitoris entirely.[4]
Reflex neurosis was a common diagnosis in the 19th century.[4] Characterized by excessive nervous stimulation, this condition could often manifest in an overstimulation of the clitoris that women would attempt to quell with masturbation.[4] Women diagnosed with reflex neurosis were often circumcised in an effort to remove the irritant.[4]
From the 1880s to 1950s, excision was often performed to prevent and treat lesbianism, masturbation, depression, hysteria, and nymphomania.[19][20] These procedures continued well into the 1970s, and were covered by Blue Cross Blue Shield Insurance until 1977.[9]
Dr. James Burt, a physician from Ohio, performed a so-called "surgery of love" on over 170 women throughout the 1960s and 1970s.[21] During the nonconsensual procedure, Burt would cut around, move, and reshape the clitoris of women who had been admitted for other operations.[21] This continued well into the 1970s, when a former coworker served witness to several of Burt's victims, and he was fired and cast out of the medical community.[21]
.jpg)
Legislative framework
Federal and state policy
As of July 2017, 26 states had passed legislation making FGM illegal.[11] Several of these states passed legislation that made it illegal to perform FGM on anyone, while federal law only protects those under 18.[3]
Performing FGM on anyone under the age of 18 became a felony in the United States with the passage of the Female Genital Mutilation Act in 1996.[10] The law was introduced by former congresswoman Pat Schroeder in October 1993.[22][23] The Female Genital Mutilation Act includes education and community outreach programs that provide information about the physical and emotional harm caused by FGM.[10][22][24] In addition to community outreach programs, the U.S. Congress also required the Department of Health and Human services to provide information for medical students about treatment recommendations.[25] Education policy was also included in the Illegal Immigration Reform and Immigrant Responsibility Act of 1996.[26] The IIRARA mandated that visa recipients from 28 high-risk countries receive culturally appropriate information on the personal and legal repercussions of FGM in the United States at or before the time of entry.[26][27] In 2013, Transport for Female Genital Mutilation Act specifically prohibited the practice of "vacation cutting", the transport of a girl outside of the United States with the intention of performing FGM.[28]
International policy
In addition to policies within the U.S., FGM has been condemned by international organizations and bodies that the U.S. is a part of. The UN's 1948 Universal Declaration of Human Rights and 1989 Convention on the Rights of the Child both include statements against the practice of FGM.[12][3][13] In 1979, the Convention on the Elimination of All Forms of Discrimination Against Women (CEDAW) required participating State parties to work to "abolish customs and practices which constitute discrimination against women".[12][28] In 1990, CEDAW's General Recommendation 14 included many suggested actions for participating State parties to eradicate FGM, including the collection of data on the prevalence of FGM, education and outreach programs to prevent and discourage FGM, incorporating information on the eradication of FGM into public health programs, and encouraging politicians and public figures to speak out against FGM.[28] In 1999, CEDAW's General Recommendation recommended that participating State parties enact laws to prohibit FGM.[28] In 2007, the United Nations Children's Emergency Fund (UNICEF) and the United Nations Population Fund (UNPF) created a joint UN initiative with the goal of ending FGM within a generation.[3] In 2015, the UN's Sustainable Development Goals included the end of practices that prevent gender equality, including FGM.[3]
Prosecutions
The first conviction of FGM in the US occurred in 2006. Khalid Adem, an Ethiopian American, was both the first person prosecuted and first person convicted for FGM in the United States. Adem, an Ethiopian immigrant, circumcised his two-year-old daughter with a pair of scissors. He was found guilty of aggravated battery and cruelty to children by the State of Georgia, which had no specific law on FGM at the time.[29][30] In 2010, Georgia successfully passed a law criminalizing FGM.[31]
In April 2017, Jumana Nagarwala, a doctor working at the Henry Ford Hospital in Detroit, was charged with allegedly performing FGM at the Burhani Medical Clinic in Livonia, Michigan.[32][33] This was the first federal prosecution for female genital mutilation in US history.[34] Nagarwala, who denied the charges, was accused of performing FGM on two girls who had traveled from Minnesota with their mothers.[32] The owners of the clinic where it was performed, Dr. Fakhruddin Attar and his wife, Farida Attar, were also arrested and charged with FGM for conspiring with Nagarwala and letting her use their clinic.[35][32]
Asylum
In 1996, Fauziya Kasinga was granted political asylum by the United States Board of Immigration Appeals.[23] Kasinga, a 19-year-old member of the Tchamba-Kunsuntu tribe of Togo, was granted asylum on the grounds that she would be at risk of FGM if she returned to her arranged marriage in Togo.[23] This set a precedent in U.S. immigration law because it was the first time FGM was accepted as a form of persecution.[36] In addition, this was the first situation in which asylum was granted based on gender.[37]
Controversy
American Academy of Pediatrics
In 2010, the American Academy of Pediatrics came under fire for advising doctors to consider offering patients the option of "a ritual nick as a possible compromise to avoid greater harm"[38] The Academy stated that although harmful genital mutilation is illegal in the United States, physicians could consider this option in countries where FGM is more widely practiced. This advice appeared in a journal section entitled "Education of patients and parents".[38] After facing backlash from medical institutions worldwide, the AAP retracted their statement. The organization also subsequently clarified in a statement released in May 2010 that it "opposes all types of female genital cutting" and "counsels its members not to perform such procedures".[39]
See also
References
- 1 2 3 4 "Female genital mutilation". World Health Organization. Retrieved 2017-11-16.
- ↑ Goldberg, Howard; Stupp, Paul; Okoroh, Ekwutosi; Besera, Ghenet; Goodman, David; Danel, Isabella (2016). "Female Genital Mutilation/Cutting in the United States: Updated Estimates of Women and Girls at Risk, 2012". Public Health Reports. 131 (2): 340–347. doi:10.1177/003335491613100218. ISSN 0033-3549. PMC 4765983. PMID 26957669.
- 1 2 3 4 5 6 Mpinga, Emmanuel Kabengele; Macias, Aurélie; Hasselgard-Rowe, Jennifer; Kandala, Ngianga-Bakwin; Félicien, Tshimungu Kandolo; Verloo, Henk; Bukonda, Ngoyi K. Zacharie; Chastonay, Philippe (2016-12-01). "Female genital mutilation: a systematic review of research on its economic and social impacts across four decades". Global Health Action. 9 (1): 31489. doi:10.3402/gha.v9.31489. ISSN 1654-9716. PMC 5052514. PMID 27707452.
- 1 2 3 4 5 6 7 8 9 Rodriguez, Sarah W. (2008-07-01). "Rethinking the History of Female Circumcision and Clitoridectomy: American Medicine and Female Sexuality in the Late Nineteenth Century". Journal of the History of Medicine and Allied Sciences. 63 (3): 323–347. doi:10.1093/jhmas/jrm044. ISSN 0022-5045.
- 1 2 3 4 5 Wagner, Natascha (2015-03-04). "Female Genital Cutting and Long-Term Health Consequences – Nationally Representative Estimates across 13 Countries". The Journal of Development Studies. 51 (3): 226–246. doi:10.1080/00220388.2014.976620. ISSN 0022-0388.
- 1 2 Goldberg, Howard; Stupp, Paul; Okoroh, Ekwutosi; Besera, Ghenet; Goodman, David; Danel, Isabella (2016). "Female Genital Mutilation/Cutting in the United States: Updated Estimates of Women and Girls at Risk, 2012". Public Health Reports. 131 (2): 340–347. doi:10.1177/003335491613100218. ISSN 0033-3549. PMC 4765983. PMID 26957669.
- 1 2 3 4 5 6 7 Goldberg, Howard; Stupp, Paul; Okoroh, Ekwutosi; Besera, Ghenet; Goodman, David; Danel, Isabella (2016). "Female Genital Mutilation/Cutting in the United States: Updated Estimates of Women and Girls at Risk, 2012". Public Health Reports. 131 (2): 340–347. doi:10.1177/003335491613100218. ISSN 0033-3549. PMC 4765983. PMID 26957669.
- 1 2 Webber, Sara; Schonfeld, Toby L. (2003-06-27). "Cutting History, Cutting Culture: Female Circumcision in the United States". The American Journal of Bioethics. 3 (2): 65–66. doi:10.1162/152651603766436324. ISSN 1536-0075.
- 1 2 Kinnear, Karen L. (2011). Women in Developing Countries: A Reference Handbook. ABC-CLIO. ISBN 9781598844252.
- 1 2 3 "18 U.S. Code § 116 - Female genital mutilation". LII / Legal Information Institute. Retrieved 2017-11-16.
- 1 2 "24 US states still have no laws against female genital mutilation. Yes, you read that right". Retrieved 2017-11-23.
- 1 2 3 "General recommendations made by the Committee on the Elimination of Discrimination against Women". www.un.org. Retrieved 2017-11-23.
- 1 2 "The United Nations Convention of the Rights of the Child: A Feminist Landmark". William & Mary Journal of Women and the Law. 3: 51.
- ↑ http://www.equalitynow.org/sites/default/files/EN_FAQ_FGM_in_US.pdf
- ↑ "Women and Girls at Risk of Female Genital Mutilation/Cutting in the United States". www.prb.org. Retrieved 2017-10-20.
- ↑ Goldberg, Howard; Stupp, Paul; Okoroh, Ekwutosi; Besera, Ghenet; Goodman, David; Danel, Isabella (2016). "Female Genital Mutilation/Cutting in the United States: Updated Estimates of Women and Girls at Risk, 2012". Public Health Reports. 131 (2): 340–347. doi:10.1177/003335491613100218. ISSN 0033-3549. PMC 4765983. PMID 26957669.
- ↑ "Nymphomania: The Historical Construction of Female Sexuality". www.brown.uk.com. Retrieved 2017-11-25.
- ↑ Degler, Carl N. (1974). "What Ought To Be and What Was: Women's Sexuality in the Nineteenth Century". The American Historical Review. 79 (5): 1467–1490. doi:10.2307/1851777. JSTOR 1851777.
- ↑ Watson, Mary Ann (2005-01-01). "Female circumcision from Africa to the Americas: Slavery to the present". The Social Science Journal. 42 (3): 421–437. doi:10.1016/j.soscij.2005.06.006.
- ↑ Studd, John; Schwenkhagen, Anneliese (2009-06-20). "The historical response to female sexuality". Maturitas. Female sexual dysfunctions in the office. 63 (2): 107–111. doi:10.1016/j.maturitas.2009.02.015.
- 1 2 3 Johnsdotter, Sara (2012). "Projected Cultural Histories of the Cutting of Female Genitalia: A Poor Reflection as in a Mirror". History and Anthropology. 23 (1): 91–114. doi:10.1080/02757206.2012.649270.
- 1 2 Ann, James, Mary (2013). "Federal Prohibition of Female Genital Mutilation: The Female Genital Mutilation Act of 1993, H.R. 3247". Berkeley Journal of Gender, Law & Justice. 9 (1). doi:10.15779/z38dk2f. ISSN 1933-1045.
- 1 2 3 Leonard, Lori (2000-03-01). "Interpreting Female Genital Cutting: Moving beyond the Impasse". Annual Review of Sex Research. 11 (1): 158–190. doi:10.1080/10532528.2000.10559787. ISSN 1053-2528.
- ↑ "Female Genital Mutilation Outlawed In United States". BMJ: British Medical Journal. 313 (7065): 1103–1103. 1996. doi:10.1136/bmj.313.7065.1103a. JSTOR 29733347.
- ↑ Horowitz, Carol R; Jackson, J Carey (August 1997). "Female "Circumcision"". Journal of General Internal Medicine. 12 (8): 491–499. doi:10.1046/j.1525-1497.1997.00088.x. ISSN 0884-8734. PMC 1497147. PMID 9276655.
- 1 2 "Notice of Implementation of the Illegal Immigration Reform and Immigrant Responsibility Act of 1996 Pertaining to Female Genital Mutilation (FGM) [63 FR 13433] [FR 20-98] | USCIS". www.uscis.gov. Retrieved 2017-11-23.
- ↑ Female genital mutilation : a guide to laws and policies worldwide. Rahman, Anika., Toubia, Nahid., Center for Reproductive Law & Policy., RAINBO (Organization). London: Zed Books. 2000. ISBN 9781856497732. OCLC 44548936.
- 1 2 3 4 Goldberg, Howard; Stupp, Paul; Okoroh, Ekwutosi; Besera, Ghenet; Goodman, David; Danel, Isabella (2016). "Female Genital Mutilation/Cutting in the United States: Updated Estimates of Women and Girls at Risk, 2012". Public Health Reports. 131 (2): 340–347. doi:10.1177/003335491613100218. ISSN 0033-3549. PMC 4765983. PMID 26957669.
- ↑ http://news.bbc.co.uk/2/hi/americas/6108516.stm
- ↑ http://usatoday30.usatoday.com/news/nation/2006-11-01-georgia_x.htm
- ↑ "2010 Georgia Code :: TITLE 16 - CRIMES AND OFFENSES :: CHAPTER 5 - CRIMES AGAINST THE PERSON :: ARTICLE 2 - ASSAULT AND BATTERY :: § 16-5-27 - Female genital mutilation". Justia Law. Retrieved 2017-11-24.
- 1 2 3 Archive, United States Courts. "United States of America v. Nagarwala et al Docket Item 16 | United States Courts Archive". www.unitedstatescourts.org. Retrieved 2017-11-24.
- ↑ "Criminal Complaint", The U.S. District Court for the Eastern District of Michigan, 12 April 2017.
- ↑ Rubin, Rita. "Doctor Charged With Female Genital Mutilation Has Published Research, Overseen Residents". Forbes. Retrieved 2017-11-24.
- ↑ Allen, Tresa Baldas and Robert. "Another doctor, wife charged with female genital mutilation in Michigan". chicagotribune.com. Retrieved 2017-11-24.
- ↑ Dugger, Celia W. "June 9-15; Asylum From Mutilation",The New York Times, 16 June 1996.
- "In re Fauziya KASINGA, file A73 476 695, U.S. Department of Justice, Executive Office for Immigration Review, decided 13 June 1996.
- Dugger, Celia W. "Woman's Plea for Asylum Puts Tribal Ritual on Trial", The New York Times, 15 April 1996.
- ↑ "Global feminism at the local level: Criminal and asylum laws regarding female genital surgeries". Journal of Gender, Race and Justice. 3: 45–62.
- 1 2 Kmietowkz, Zosia (22 May 2010). "UK colleges criticise US advice on female genital mutilation". BMJ: British Medical Journal. 340: 1103. JSTOR 40702226.
- ↑ "Ritual Genital Cutting of Female Minors". Pediatrics. Retrieved 13 October 2017.
Further reading
- Abdelkader E, Abugideiri SE, Diallo M (2014). "Female Genital Mutilation In The United States". Islamic Horizons. 43 (5): 36–38.
- Jones WK, Smith J, Kieke B Jr, Wilcox L (1997). "Female genital mutilation. Female circumcision. Who is at risk in the U.S.?". Public Health Reports. Association of Schools of Public Health. 112 (5): 368–377. PMC 1381943. PMID 9323387.
- McConnell, Kathryn (7 February 2013). "U.S. Taking Steps to Stop Female Genital Mutilation". IIP Digital. U.S. Department of State. Retrieved 8 December 2014.