Vestibular system
The vestibular system, in most mammals, is the sensory system that provides the leading contribution to the sense of balance and spatial orientation for the purpose of coordinating movement with balance. Together with the cochlea, a part of the auditory system, it constitutes the labyrinth of the inner ear in most mammals. As movements consist of rotations and translations, the vestibular system comprises two components: the semicircular canals which indicate rotational movements; and the otoliths which indicate linear accelerations. The vestibular system sends signals primarily to the neural structures that control eye movements, and to the muscles that keep an animal upright. The projections to the former provide the anatomical basis of the vestibulo-ocular reflex, which is required for clear vision; and the projections to the muscles that control posture are necessary to keep an animal upright.
The brain uses information from the vestibular system in the head and from proprioception throughout the body to understand the body's dynamics and kinematics (including its position and acceleration) from moment to moment.
Semicircular canal system
The semicircular canal system detects rotational movements. The semicircular canals are its main tools to achieve this detection.
Structure
Since the world is three-dimensional, the vestibular system contains three semicircular canals in each labyrinth. They are approximately orthogonal (at right angles) to each other, and are the horizontal (or lateral), the anterior semicircular canal (or superior), and the posterior (or inferior) semicircular canal. Anterior and posterior canals may collectively be called vertical semicircular canals.
- Movement of fluid within the horizontal semicircular canal corresponds to rotation of the head around a vertical axis (i.e. the neck), as when doing a pirouette.
- The anterior and posterior semicircular canals detect rotations of the head in the sagittal plane (as when nodding), and in the frontal plane, as when cartwheeling. Both anterior and posterior canals are orientated at approximately 45° between frontal and sagittal planes.
The movement of fluid pushes on a structure called the cupula which contains hair cells that transduce the mechanical movement to electrical signals.[1]
Push-pull systems
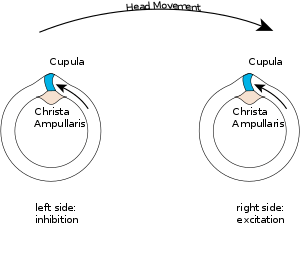
The canals are arranged in such a way that each canal on the left side has an almost parallel counterpart on the right side. Each of these three pairs works in a push-pull fashion: when one canal is stimulated, its corresponding partner on the other side is inhibited, and vice versa.
This push-pull system makes it possible to sense all directions of rotation: while the right horizontal canal gets stimulated during head rotations to the right (Fig 2), the left horizontal canal gets stimulated (and thus predominantly signals) by head rotations to the left.
Vertical canals are coupled in a crossed fashion, i.e. stimulations that are excitatory for an anterior canal are also inhibitory for the contralateral posterior, and vice versa.
Vestibulo-ocular reflex (VOR)
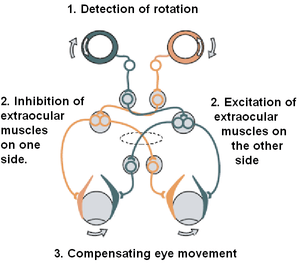
The vestibulo-ocular reflex (VOR) is a reflex eye movement that stabilizes images on the retina during head movement by producing an eye movement in the direction opposite to head movement, thus preserving the image on the center of the visual field. For example, when the head moves to the right, the eyes move to the left, and vice versa. Since slight head movements are present all the time, the VOR is very important for stabilizing vision: patients whose VOR is impaired find it difficult to read, because they cannot stabilize the eyes during small head tremors. The VOR reflex does not depend on visual input and works even in total darkness or when the eyes are closed.
This reflex, combined with the push-pull principle described above, forms the physiological basis of the Rapid head impulse test or Halmagyi-Curthoys-test, in which the head is rapidly and forcefully moved to the side while observing whether the eyes keep looking in the same direction.
Mechanics
The mechanics of the semicircular canals can be described by a damped oscillator. If we designate the deflection of the cupula with , and the head velocity with , the cupula deflection is approximately



α is a proportionality factor, and s corresponds to the frequency. For humans, the time constants T1 and T2 are approximately 3 ms and 5 s, respectively. As a result, for typical head movements, which cover the frequency range of 0.1 Hz and 10 Hz, the deflection of the cupula is approximately proportional to the head-velocity. This is very useful, since the velocity of the eyes must be opposite to the velocity of the head in order to have clear vision.
Central processing
Signals from the vestibular system also project to the cerebellum (where they are used to keep the VOR effective, a task usually referred to as learning or adaptation) and to different areas in the cortex. The projections to the cortex are spread out over different areas, and their implications are currently not clearly understood.
Projection pathways
The vestibular nuclei on either sides of the brain stem exchange signals regarding movement and body position. These signals are sent down the following projection pathways.
- To the cerebellum. Signals sent to the cerebellum are relayed back as muscle movements of the head, eyes, and posture.
- To nuclei of cranial nerves III, IV, and VI. Signals sent to these nerves cause the vestibulo-ocular reflex. They allow for the eyes to fix on a moving object while staying in focus.
- To the reticular formation. Signals sent to the reticular formation signal the new posture the body has taken on, and how to adjust circulation and breathing due to body position.
- To the spinal cord. Signals sent to the spinal cord allow quick reflex reactions to both the limbs and trunk to regain balance.
- To the thalamus. Signals sent to the thalamus allow for head and body motor control as well as being conscious of body position.[2]
- Via the Ventral Pathway, which contributes to vertical orientation and perception of the direction of gravity.[3]
Otolithic organs
While the semicircular canals respond to rotations, the otolithic organs sense linear accelerations. Humans have two otolithic organs on each side, one called the utricle, the other called the saccule. The utricle contains a patch of hair cells and supporting cells called a macula. Similarly, the saccule contains a patch of hair cells and a macula. Each hair cell of a macula has 40-70 stereocilia and one true cilium called a kinocilium. The tips of these cilia are embedded in an otolithic membrane. This membrane is weighted down with protein-calcium carbonate granules called otoliths. These otoliths add to the weight and inertia of the membrane and enhance the sense of gravity and motion. With the head erect, the otolithic membrane bears directly down on the hair cells and stimulation is minimal. When the head is tilted, however, the otolithic membrane sags and bends the stereocilia, stimulating the hair cells. Any orientation of the head causes a combination of stimulation to the utricles and saccules of the two ears. The brain interprets head orientation by comparing these inputs to each other and to other input from the eyes and stretch receptors in the neck, thereby detecting whether the head is tilted or the entire body is tipping.[2] Essentially, these otolithic organs sense how quickly you are accelerating forward or backward, left or right, or up or down.[4] Most of the utricular signals elicit eye movements, while the majority of the saccular signals projects to muscles that control our posture.
While the interpretation of the rotation signals from the semicircular canals is straightforward, the interpretation of otolith signals is more difficult: since gravity is equivalent to a constant linear acceleration, one somehow has to distinguish otolith signals that are caused by linear movements from those caused by gravity. Humans can do that quite well, but the neural mechanisms underlying this separation are not yet fully understood. Humans can sense head tilting and linear acceleration even in dark environments because of the orientation of two groups of hair cell bundles on either side of the striola. Hair cells on opposite sides move with mirror symmetry, so when one side is moved, the other is inhibited. The opposing effects caused by a tilt of the head cause differential sensory inputs from the hair cell bundles allow humans to tell which way the head is tilting,[5] Sensory information is then sent to the brain, which can respond with appropriate corrective actions to the nervous and muscular systems to ensure that balance and awareness are maintained.[6]
Experience from the vestibular system
Experience from the vestibular system is called equilibrioception. It is mainly used for the sense of balance and for spatial orientation. When the vestibular system is stimulated without any other inputs, one experiences a sense of self-motion. For example, a person in complete darkness and sitting in a chair will feel that he or she has turned to the left if the chair is turned to the left. A person in an elevator, with essentially constant visual input, will feel she is descending as the elevator starts to descend. There are a variety of direct and indirect vestibular stimuli which can make people feel they are moving when they are not, not moving when they are, tilted when they are not, or not tilted when they are.[7] Although the vestibular system is a very fast sense used to generate reflexes, including the righting reflex, to maintain perceptual and postural stability, compared to the other senses of vision, touch and audition, vestibular input is perceived with delay.[8][9]
Vestibular/somatogyral illusions
Pathologies
Diseases of the vestibular system can take different forms, and usually induce vertigo[10] and instability or loss of balance, often accompanied by nausea. The most common vestibular diseases in humans are vestibular neuritis, a related condition called labyrinthitis, Ménière's disease, and BPPV. In addition, the function of the vestibular system can be affected by tumors on the vestibulocochlear nerve, an infarct in the brain stem or in cortical regions related to the processing of vestibular signals, and cerebellar atrophy.
Alcohol can also cause alterations in the vestibular system for short periods and will result in vertigo and possibly nystagmus due to the variable viscosity of the blood and the endolymph during the consumption of alcohol. The common term for this type of sensation is the bed spins.
- PAN I - The alcohol concentration is higher in the blood than in the vestibular system, hence the endolymph is relatively dense.
- PAN II - The alcohol concentration is lower in the blood than in the vestibular system, hence the endolymph is relatively dilute.
PAN I will result in subjective vertigo in one direction and typically occurs shortly after ingestion of alcohol when blood alcohol levels are highest. PAN II will eventually cause subjective vertigo in the opposite direction. This occurs several hours after ingestion and after a relative reduction in blood alcohol levels.
Benign paroxysmal positional vertigo, or BPPV for short, is a condition resulting in acute symptoms of vertigo in people. It is probably caused when pieces that have broken off otoliths have slipped into one of the semicircular canals. In most cases it is the posterior canal that is affected. In certain head positions, these particles shift and create a fluid wave which displaces the cupula of the canal affected, which leads to dizziness, vertigo and nystagmus.
A similar condition to BPPV may occur in dogs and other mammals, but the term vertigo cannot be applied because it refers to subjective perception. Terminology is not standardized for this condition.
A common vestibular pathology of dogs and cats is colloquially known as "old dog vestibular disease", or more formally idiopathic peripheral vestibular disease, which causes sudden episode of loss of balance, circling, head tilt, and other signs. This condition is very rare in young dogs but fairly common in geriatric animals, and may affect cats of any age.[11]
Vestibular dysfunction has also been found to correlate with cognitive and emotional disorders, including depersonalization and derealization.[12]
See also
References
- ↑ Boulpaep, Emile L.; Boron, Walter F. (2005). Medical physiology: a cellular and molecular approach. St. Louis, Mo: Elsevier Saunders. ISBN 1-4160-2328-3. OCLC 56963726.
- 1 2 Saladin, Kenneth S. (2011). Anatomy & Physiology: The Unity of Form and Function. New York: McGraw-Hill. ISBN 0-07-337825-9. OCLC 799004854.
- ↑ Vaziri, Siavash; Connor, Charles E (2016). "Representation of Gravity-Aligned Scene Structure in Ventral Pathway Visual Cortex". Current Biology. 26: 766–74. doi:10.1016/j.cub.2016.01.022. PMC 4819394. PMID 26923785. Lay summary.
... the ventral pathway, ...could support perceiving and/or predicting physical events involving objects subject to gravity ...
- ↑ "The Physiology of the Senses: Balance" (PDF).
- ↑ "The Otolith Organs: The Utricle and Sacculus". NCBI Bookshelf - Neuroscience.
- ↑ Angelaki DE, Cullen KE (2008). "Vestibular system: the many facets of a multimodal sense". Annu. Rev. Neurosci. 31: 125–50. doi:10.1146/annurev.neuro.31.060407.125555. PMID 18338968.
- ↑ Lawson, B. D., & Riecke, B. E. (2014). The Perception of Body Motion. Handbook of Virtual Environments, CRC Press, 163-196.
- ↑ Barnett-Cowan, M., and Harris, L. R. (2009), Perceived timing of vestibular stimulation relative to touch, light and sound. Experimental Brain Research, 198: 221-231. "doi: 10.1007/s00221-009-1779-4".
- ↑ Barnett-Cowan, M. (2013), Vestibular perception is slow: a review. Multisensory Research, 26: 387-403. "doi: 10.1163/22134808-00002421".
- ↑ "Vertigo". University of Maryland Medical Center. Retrieved 13 November 2015.
- ↑ Rossmeisl, John (2010). "Vestibular Disease in Dogs and Cats". Veterinary Clinics of North America: Small Animal Practice. 40 (1): 80–100. doi:10.1016/j.cvsm.2009.09.007. Retrieved 12 March 2017.
- ↑ Smith, Paul F; Darlington, Cynthia L (2013). "Personality changes in patients with vestibular dysfunction". Frontiers in Human Neuroscience. 7: 678. doi:10.3389/fnhum.2013.00678. PMC 3810789. PMID 24194706. Lay summary.
patients with vestibular disorders have been reported to experience other personality changes that suggest that vestibular sensation is implicated in the sense of self. These are depersonalization and derealization symptoms such as feeling "spaced out", "body feeling strange" and "not feeling in control of self". We propose in this review that these symptoms suggest that the vestibular system may make a unique contribution to the concept of self through information regarding self-motion and self-location that it transmits, albeit indirectly, to areas of the brain such as the temporo-parietal junction
Further reading
- S. M. Highstein, R. R. Fay, A. N. Popper, editors (2004). The vestibular system. Berlin: Springer. ISBN 0-387-98314-7. OCLC 56068617. (Comment: A book for experts, summarizing the state of the art in our understanding of the balance system)
- Thomas Brandt (2003). Vertigo : Its Multisensory Syndromes. Berlin: Springer. ISBN 0-387-40500-3. OCLC 52472049. (Comment: For clinicians, and other professionals working with dizzy patients.)
- "Driver Fatigue: Is Something Missing?" (pdf). Christopher Brill, Peter A. Hancock, Richard D. Gilson - University of Central Florida - 2003. (Comment: Research on driver or motion-induced sleepiness aka 'sopite syndrome' links it to the vestibular labyrinths.)
- Vestibular system Kathleen Cullen and Soroush Sadeghi, Scholarpedia, 3(1):3013. doi:10.4249/scholarpedia.3013
- A preview of an article on how vestibular disorders can cause symptoms that look like mental disorders.
External links
- Vestibular Disorders Association For more information about vestibular (inner ear balance) disorders.
- (Video) Head Impulse Testing site (vHIT) Site with thorough information about vHIT
- SensesWeb, which contains animations of all sensory systems, and additional links.
- Dizzytimes.com Online Community for Sufferers of Vertigo and Dizziness.
- Vestibular System, Neuroscience Online (electronic neuroscience textbook)